|
|
|
|
Patient Centered Teaching.
Patient Centered Research.
Patient Centered Care. |
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From the Desk of Dr. Sinnott... |
|
We are three months into the new academic year and I cannot be prouder of the progress you all are making.
As internal and external environmental factors are continually changing, I am impressed with how quickly we are able to adapt to so many changes while still making progress toward our goals.
Some exciting changes include the search for a new VP of USF Health and Dean of Morsani College of Medicine and the Tampa General Hospital partnership with Florida Hospital Systems. In addition, the Affordable Care Act has been implemented, which will bring a change to the entire health system as we know it.
The search committee for the new dean has interviewed 2 candidates, and consists of 5 external candidates and 4 internal as of Oct 7th. We are in the process of interviewing the candidates and have to have a decision by Christmas. Thank you to the 60 people who completed our survey. Ours was the only faculty survey of suggestions, and your input was integral to shaping the decision process. Thank you for your insight and great ideas.
The chairman's office is working hard to build the infrastructure we need to ensure you get timely news and information as it happens. We are also working on ways we can make operations more integrated. One example is the One Stop Shopping Survey you all completed, and we are aggregating the results now. We started out simply to see what we could consolidate or make easier for the faculty and have ended up with an astounding array of answers. As these new ways are instituted, we will ensure you are properly informed and trained/supported in how to use them.
From professional enrichment seminars on the Affordable Care Act, to news blasts and intranets to pool and share resources, I hope you are confident that we are doing all we can to support you and live up to our commitment to making the USF Department of Internal Medicine a great place to work.
Warmly,
John
John T Sinnott MD FACP
Chairman
Department of Internal Medicine
|

Inside This Issue...
|
|
|
|
|
Patient Centered Teaching
Our New Physicians Assistant Program approved by BOT and slated to accept first class in 2014. Learn more.
|
Patient Centered Research
Ben Djulbegovic, MD, PhD shares the future direction of the new Division of Evidence Based Medicine. Learn more.
|
Patient Centered Care
Pallavi and Kiran Patel help us improve international medicine through our new IM Sustainable program. Learn more.
|
|
|
|
|
|
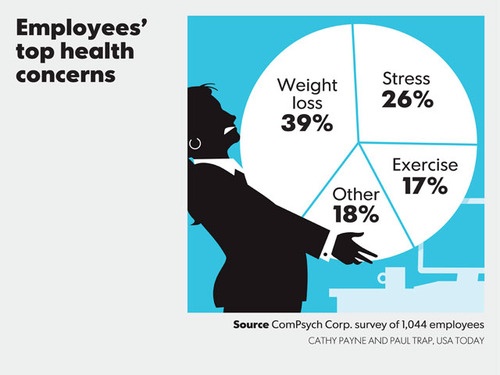
Employee Health and Wellness
Results from our Cholesterol Screening and first fitness challenge. Learn more.
|
ACA Top 10 By Robert Brooks
Robert Brooks, MD, MBA, MPH breaks down what you should know about the ACA. Learn more.
|
|
|
|
|
|
|
Professional Enrichment Seminar
Come learn how to safeguard yourself from identity theft Wed Oct 30th 6pm TGH B107. Learn more.
|
Grand Rounds Schedule
View the upcoming Grand Rounds Lectures schedule here.
|
Meet our New Hires
We've hired many hospitalists, researchers and faculty. Meet the team!
|
|
ANNOUNCEMENTS & IMPORTANT INFO
|
|
Has the IM Cares program helped you in any way? Share with others!Send in your stories of how it benefited you, and your comments could be highlighted on our Web site, annual report, and Facebook page!
|
| |
Cholesterol Screening Results
The end of September our third year medical students Michael Cameron and Jae Chung visited our offices to provide total cholesterol checks and random glucose levels.
Here are the results:
-
25 employees screened for Total Cholesterol and Random Glucose Levels
-
3 employees with High Total Cholesterol Level (240 mg/dL and above)
-
5 employees with Borderline High Total Cholesterol Level (200-239 mg/dL)
-
0 employees with Diabetes (Glucose 200 mg/dL and above)
-
0 employees with Prediabetes (Glucose 140 to 199 mg/dL and above)
Employees with elevated cholesterol were encouraged to seek further testing and possible treatment from their primary care physician.
For those who missed the screening or would like to be retested, we plan to hold another cholesterol screening in the Spring.
|
We just completed our first DOIM Battle of the Bulge Summer Slimdown Fitness Challenge!
Twenty faculty and staff members in our department participated in our first fitness challenge.
From July 1 - August 30, six teams of 3-4 people worked together to improve their overall health and fitness, with a core focus on reducing overall body fat percentages.
We lost a combined 61 lbs, 33.57% of body weight, 34 inches, and 8.1% of body fat!
Congratulations to team Carolyn Dawson, Babarba Pearce and Julie DeHainaut who lost the most: 29.8lbs, 24.5 inches, and 6.6% of their bodyweight!
|
|
OUR LATEST ACHIEVEMENTS
 | | Dr. Doug Holt being interviewed with Magic Johnson |
In the News
Promotions
Helen Bateman, MD (VA) Promoted to Associate Professor (Rheumatology)
 | | National attention for new initiative with Magic Johnson |
Dwight Achong, MD (VA) Promoted to Professor (Nuclear Medicine)
William Bond, MD (LVHN) Promoted to Professor (Emergency Medicine)
Marna Greenberg, DO (LVHN) Promoted to Associate Professor (Emergency Medicine)
Publications
The American Lung Association is funding our Asthma Clinical Research Center for its participation in the network's "Smoking in Asthmatic Pilot Study" (SAPS) trial (Allergy & Immunology)
Shyam Mohapatra, PhD and Subbiah Alwarappan, PhD - Licensing of Method of DNA Sensing on Graphene Platforms, USF #12B116 (Translational Medicine)
Charurut Somboonwit, MD from Division of Infectious Disease & International Medicine, appointed to the Appointment, Promotion and Tenure Committee for Oct 1, 2013-Sept 30 2016.
David Ecker, MD from Division of Hospital Medicine, appointed to serve on the Professional Student Affairs Committee for Oct 1 2013 - Sept 30, 2015
Narasaiah Kolliputi, PhD from Division of Allergy & Immunology appointed to serve on the Research Committee Oct 1 2013 - Sept 30, 2015
Kellee Oller, MD from Hospital Medicine appointed to serve on the Continuing Professional Development Committee from Oct 1 2013 - Sept 30 2016
Lady Washington, Fiscal & Business Analyst for DOIM and Administrator for Division of Translational Medicine, elected to the A&P Council for the 2013-2016. As a member, she reviews, revises, and provides recommendations for all USF System policy, procedures and employee concerns to President Genshaft's cabinet.
On August 23rd, the General Internal Medicine clinic at Morsani said goodbye to Mitchel Seleznick, MD. After 27 years with USF, Dr. Seleznick is joining Care Plus as their new Medical Director. The clinic faculty and nurses brought lunch with cake, ice cream and farewell gifts. Dr. Sinnott presented Dr. Seleznick with a plaque for his years of service to the university.

We wish you much success in your new endeavors Dr. Seleznick!
|
|
Warm Welcome to the Newest Members of the Department of Internal Medicine
Allergy & Immunology
Young Cho, Researcher 
Eileen Rifkin, Researcher
Endocrinology and Metabolism
Sophie Hussey PhD, Researcher (Post Doctoral Scholar)
John Malone MD, Faculty (Professor)
Evidence Based Medicine
Yessenia Keith, Administrative Specialist
Hematology/Oncology
Damian Laber MD, Division Director (Professor)
Nathan Visweshwar MD, Faculty (Assistant Professor)
Hospice & Palliative Medicine
Lindsey Davidson, Graduate Research Assistant
Hospital Medicine
Anna Fountain MD, Faculty (Assistant Professor)
Cairine McNamee MD, Faculty (Assistant Professor)
Melissa Newman DO, Faculty (Assistant Professor)
Anh Nguyen DO (Assistant Professor)
Elimarys Perez-Colon MD (Assistant Professor)
Jose Rodriguez-Castillo MD (Assistant Professor)
Infectious Disease & International Medicine
Jamie Morano MD, Faculty (Assistant Professor)
Obesity, Diabetes & Aging Research Center
Cassandra Mary Nicotra, Research Assistant
Monica Segura, Research Assistant
Pulmonary
Emilie Foltz MBA, Education Coordinator
Rheumatology
Yih Chang Chen Lin MD, Faculty (Assistant Professor)
Translational Medicine
He Li, Research Associate
|
PERSONAL GROWTH & PROFESSIONAL ENRICHMENT
|
|
ENRICHMENT SEMINAR: IDENTITY THEFT - Wed. Oct 30th @ 6pm - TGH B107
 Did you know Florida is the top state for Identity Theft? Did you know Florida is the top state for Identity Theft?
Learn how to safeguard yourself!
Our second enrichment seminar will focus on how to safeguard yourself from identity theft.
Presented by: Anthony Lespada
Wenesday Oct 30th 6pm
Dinner will be provided
TGH B107
Anthony Lespada is a practicing member of the Florida Bar, the US District Court for the Middle District of Floirda; the District of Columbia Bar, the Court of Appeals for the 5th and 11th Circuit and the US Supreme Court.
His practice deals primarlily in civil and criminal tax litigation as well as general civil litigation and white collar crimes. He received an AV rating with Martindale Hubbell, the highest rating an attorney can attain. He was name one of Tampa Bay's top lawyers by Tampa Bay Magazine in 2010.
IF YOU PLAN ON ATTENDING PLEASE RSVP [email protected] TO ENSURE WE HAVE ENOUGH FOOD.
|
|
THE AFFORDABLE CARE ACT: TOP 10 THINGS YOU SHOULD KNOW
Confused about all the information swirling around the country regarding the Affordable Care Act (ACA)? Well, don't feel alone.
Over one-half of Americans in a recent poll felt they did not have enough information about the ACA to understand what it does or what is required of them personally. This despite (or because of!) the hundreds of millions of dollars spent on advertising and marketing since the bill became law in March of 2010.
These last two months have seen an upsurge in information in an attempt to prepare consumers for the official opening of the Health Insurance Exchanges on October 1st. The airwaves and web have been flooded with an almost hourly check-up on how the Exchanges are working, and how people are responding to the new opportunity to sign up for health insurance.
Cutting through the "hype" or "spin" to get to the core issues of health care reform under the ACA is important not just for consumers, but for us as physicians and other health providers, too.
Patients and their families are now beginning to regularly seek advice from their doctors and providers on what they should do about this nebulous health reform. This, therefore, seems like an opportune time to revisit some of the key provisions of the ACA. For this article I've chosen 10 of the most common and important areas of the ACA to reflect on, as they also happen to be some of the most misunderstood areas of concern to patients as well as well as physicians.

1. What is the "individual mandate", or, who is it that must have health insurance? Well, essentially all persons who are American citizens or permanent residents of the U.S. There are, however, a few important exceptions. For example, American Indians, prisoners, those who don't have to even file a federal tax return, and undocumented immigrants, are all exempt from the individual mandate for health insurance, that for everyone else will begin on January 1, 2014.
2. What if I already have health insurance? Persons who are already covered by Medicare, Medicaid, Children's Health Insurance Program (CHIP, or Title XXI), or a qualified health plan, do not have to do anything new (other than renew their current plan during the yearly open enrollment period). Most, but not all, current private insurance will remain in effect. There are cases where a health insurance plan has not had the minimal essential health benefits required under the ACA. In these cases the plans will have to change their benefits, or else not be eligible to qualify for purposes of the ACA's rules, or participate in the new Health Insurance Exchanges.
3. What if I can't afford health insurance? There are subsidies available for persons that qualify. These are based on a "sliding scale" of income. People that make either individually or as a family up to as much as 400% of the federal poverty level (note: for 2013 this was $45,960 for an individual; $94,200 for a family of four) may qualify to have their health insurance premiums either fully or partially subsidized. Since the subsidy is also related to other factors (eg. age, geographic location, tobacco use), its best to go to an independent website, such as the Kaiser Family Foundation (www.kff.org), to get an estimate of your particular subsidy eligibility and approximate amount.
4. What happens if I don't get health insurance coverage by 2014? Unless you are in one of the exempt categories noted above, you will receive a penalty. The penalty amount is based on your total yearly income and the number of people in your family. Some have noted that even the maximum possible penalty for not having individual health insurance is actually much less than the cost of buying health insurance policies in many cases, which might cause some people to choose purposely to pay the fine (and not get coverage).
5. If I get health insurance will that cover all my medical expenses? Unfortunately, no. In fact the health insurance industry has been given a set of benchmarks to meet for different levels of insurance called, bronze, silver, gold, and platinum plans. If, for example, a person chooses a bronze plan, it is actually set up to cover 60% of total yearly health care costs for that individual. By comparison, the platinum plans cover about 90% of total costs. Also of note, persons that are younger than age 30, can choose a category called catastrophic coverage. As the name suggests, it would have high deductibles and other out of pocket costs, but would be expected to kick-in with a major medical illness or injury.
6. Where do I find out about health insurance options that might be available to me? While eligible persons can buy health insurance on the open market, most of the recent attention has focused on the Health Information Exchanges (HIE). These are state-based websites that help consumers compare health insurance policies. Thirty-six states have opted to have the federal government build and run these HIEs (including Florida); 14 states are handling their own HIEs. The federal government has just opened their website (www.healthcare.gov) which has information and links to help with the important decisions about which plan may be best for you, or your patients.
7. Do all employers have to offer health insurance now? No. This is a very frequently misunderstood aspect of the ACA law. Only employers who have more than 200 employees are actually required to offer them a qualifying health insurance plan. Employers that have between 50 and 200 employees have to offer health insurance OR pay a penalty. This penalty is $2,000 per employee (after the first 30 employees). Interestingly, this penalty is again much less than the average cost of actually buying insurance (over $15,000 per year for an employee and family of four), leading some businesses to decide to either not provide health insurance, or to even drop coverage that they had already offered. Additionally, this requirement of the ACA has been delayed by the administration in Washington until 2015, leaving the odd and undesired situation where individuals are required to have health insurance coverage (by Jan. 1, 2014), but these employers are not required to offer it until 2015. Also of note, employers with less than 50 employees (who make up most businesses in the U.S.) are NOT required to offer health insurance under the ACA.
8. What impact will the ACA have on Medicare? There are a number of provisions of the ACA that deal with important aspects of Medicare. The ACA will phase out the part of Medicare drug costs that is known as the "donut hole." This is the part of Medicare drug coverage that currently results in patients having to pay 100% of their prescription drug costs once their yearly drug expenses reach a certain amount. Seniors will be pleased to have this somewhat confusing aspect of Medicare phased out by 2019. The ACA also builds on earlier work on what are called "bundled" payment models, to expand to what are now called Accountable Care Organizations (ACOs). This trend towards paying for whole episodes of care will result in doctors and hospitals working more closely together to ultimately result in better quality of care for seniors at a lower total price to them and to taxpayers. Another important aspect related to Medicare is decreased funding for Medicare Advantage plans under the ACA. This sizable decrease in payments could potentially effect the many Medicare patients (note: about 33% of all Medicare patients in Florida) who get their care through managed care- usually an HMO or PPO. To adapt these plans may have to decrease coverage benefits, or even leave a geographic area completely.
9. What impact will the ACA have on Medicaid? Probably the single largest impact of the ACA on the Medicaid program is the expansion of access to care. States have been given the option to expand their Medicaid programs to all persons who make less than 138% of the federal poverty level (2013: $15,856 for an individual) in that state. Approximately one-half of the states have chosen to expand Medicaid access; one-half (including Florida) have not. If this expansion does occur in Florida in the future, it would add between 1 - 1.2 million new persons on to our Medicaid program. A second area that relates to Medicaid is the ACA provision that increases the pay for primary care physicians who care for Medicaid patients up to the "Medicare level." While this pay increase is only guaranteed for two years (2013 and 2014), it will stimulate much needed access to care for current Medicaid persons.
10. So, after all this (and much more that we didn't have space to discuss) what does the ACA mean for the future of health and health care in the U.S.? Probably most important to understand is that the ACA law is primarily focused on increasing access to care through new insurance mandates and focus. While there are some good provisions that relate to prevention and quality, many health economists in the country have expressed concern that even with the original plan of adding 32 million additional Americans to the health insurance market (18 million through expanded Medicaid; most of the rest through the health care marketplace) the bill doesn't do enough to "bend the cost curve", that is, to really address why health care costs are so high in the U.S. Nonetheless, this, the largest change to the U.S. health care system in almost 50 years, will take a step towards having more people covered, a step that is known to improve quality of life. There are concurrently parts of the law which require revisiting and reshaping, and more attention will need to be given to areas such as the health care workforce needed to care for these new patients. Even with this, our challenge as physicians and health care providers will be to continue to provide high quality cost-effective health care services for our individual patients, while continuing to advocate for a much needed national debate on the why of health care cost increases.
|
 Grand Rounds Lecture Schedule
Thursday, October 24th
HIV Highlights for Internists
By: Charurut Somboonwit, MD
Infectious Disease
Thursday, October 31st
A Focus on Angioedema: Key Insights in Diagnosis and Management
By: Richard F Lockey, MD, FACP
Division Director, Allergy & Immunology
Thursday, November 7th
Heparin Induced Thrombocytopenia
Awareness Can Save Lives
By: Damian Laber, MD, FACP
Division Director, Hematology/Oncology
Thursday, November 14th
TBA
Thursday, November 21st
TBA
*All DoIM Grand Rounds lectures are held from noon - 1:00pm in MDL 1003, lunch is provided. They are televised at TGH B107 and FOB 1304.
|
Faculty and Staff Spotlights
|
|
Patient-Centered Teaching: Preparing Tomorrow's Leaders
|
Our New Physicians Assistant Program is Approved: Slate to Accept the First Class of Students in 2015
Twenty-four students by summer 2015.
 | |
Dave Kotun, PA-C, EdD, Program Director
|
That's the first target for David Kotun, PA-C, EdD, Program Director.
Second and third marks for the founding director of USF's Physician Assistant (PA) degree program are to build a program that helps meet the high demand for primary care professionals, and to offer a viable career opportunity for the many veterans in the USF System and the Tampa Bay area.
"The need for more primary care providers is acute, and the transition into the Affordable Care Act will increase the demand even more," Dr. Kotun said. "To help meet that demand, we'll be mirroring the national push and the roots of our profession to consider our returning veterans who gained medical and healthcare experience while serving."
The USF Board of Trustees approved plans March 21 to establish the program. The only other public university master's-level PA program in Florida is currently offered by the University of Florida. The approval was an important step forward in helping address the state's increasing shortage of primary care practitioners.
"We already have strong interest from our own USF undergraduate students in physician assistant programs, but in the past we've had to send these highly qualified students to other programs in Florida.," said Stephen K. Klasko, MD, MBA, former dean of the Morsani College of Medicine and CEO of USF Health. We feel this program will rapidly become recognized as a national leader for its innovative approach.It is a great addition to our health offerings and is a natural philosophic fit for our commitment to interprofessional education and interdisciplinary cooperation,"
The first class for the two-year PA program will start the summer of 2015, pending provisional accreditation from the ARC-PA (our national accrediting body), initially accepting 24 students. We expect to eventually enroll up to 50 to 60 PA students a year.
Our program is a few months shorter than some other PA programs in the state, focusing the first year on didactic learning and the second on clinical education, with mandatory rotations in:
- family medicine
- internal medicine
- general surgery
- pediatrics
- women's care, and
- emergency department
It will feature elective courses in mental health patient management and technical and procedural-based interventions. It will build upon USF Health's already strong foundations other disciplines and provide co-learning with medical, nursing, pharmacy, athletic training, and physical therapy.
"A magical thing happens when you get PA students together with students from other disciplines, then task them with reaching a diagnosis," said Kotun. "Attacking the problem via a different set of experiences, education, and skills leads to innovation and new ideas that bring our medical care skills to a truly high level."
Our PA graduates will be generalists for the first few years, but there might be opportunities to get post-graduate fellowships for specialties in future years.
Next Steps: to assure the program is on target for accreditation by the Accreditation Review Commission on Education for the Physician Assistant (ARC-PA).
That process starts with earning provisional accreditation, which in and of itself has three steps:
- a feasibility study to show how well this institution can support the program was submitted in August 2013
- submission of a comprehensive application that gets into specifics, like the number of people supporting the program, the clinical experience, curriculum, clinical rotations, etc. (due in December), and
- an ARC-PA team visit to confirm the program's offerings (set for February).
Then the ARC-PA meets in September 2014, taking about 30 days to review applications in detail and determine approval.
 | | Dr. Alicia Monroe, Vice Dean for Educational Affairs and Dave. |
Although Dr. Kotun is building a new program, he's quick to point out he's using the foundation laid by a wonderful team of USF Health faculty and administrators. "I cannot take the credit for where we are now with this PA program," Dr. Kotun said. "It's Stephen Klasko, Gretchen Koehler, Alicia Monroe, Larry Collins, Toni Anderson, and Allan Goldman. They all worked very hard to build the program to the point when I came in. I'm just continuing their work from here."
Alicia Monroe, MD, Vice Dean for Educational Affairs at the Morsani College of Medicine; Gretchen Koehler, PhD, Assistant Dean for Academic Administration; and Larry Collins, PA-C, ATC, an Assistant Professor of orthopaedics and sports medicine, were instrumental in helping to develop the new program. Collins will be one of the PA faculty members.
Dr. Kotun is already reaching out to veterans, having connected with the USF Office of Veteran's Affairs for recruiting USF undergraduates, as well as contacting both the Haley VA and Bay Pines VA hospitals for providing information about the PA program to the veterans being seen at the two hospitals and rehab programs.
About Our Faculty: David Kotun
Dr. Kotun earned his doctorate in Higher Education Leadership from USF, and worked as physician assistant in the USF Department of Family Medicine. Prior to joining USF, Dr. Kotun was the director of clinical education for Nova Southeastern University's four physician assistant programs at Nova Southeastern University while based in Orlando.
Photos by Eric Younghans, USF Health Communications
|
|
Patient-Centered Research: Innovative Ideas
|
|
Distinguished Professor Benjamin Djulbegovic, MD, PhD Strengthens Research of the DOIM Through Efforts of the New Division of Evidence Based Medicine
 We live in an unprecedented time dominated by a paradox: more money is spent on health care research, development and delivery, and yet health outcomes, quality of care and quality of research is by all measures considered suboptimal (In fact, 30-50% and 85% of investment health care and research, respectively, amount to the waste). We live in an unprecedented time dominated by a paradox: more money is spent on health care research, development and delivery, and yet health outcomes, quality of care and quality of research is by all measures considered suboptimal (In fact, 30-50% and 85% of investment health care and research, respectively, amount to the waste).
Research over the last decade has identified two key reasons for such unsatisfactory situation:
1) Suboptimal health care outcomes can mostly relate to the lack of high quality evidence on the effects of most interventions. This is due in large part to severe problems with the clinical research system that mostly generates poor clinical evidence.
2) The second key reason for suboptimal health outcomes relates to inferior decision-making. In fact, it has been demonstrated that "poor decision-making is responsible for the majority of deaths" in the U.S.
Another unprecedented characteristic of our times is that we are now on the verge of accomplishing a century old dream: full integration of research, education/mentoring and clinical practice. Institutions not successful in accomplishing this integration that fail to measure the effects of their efforts will be sorely left behind.
Solutions to the identified challenges above are:
1) strengthen the reliability of the evidence base by improving the science of clinical research, and
2) to improve decision-making, enabling translating research into practice by delivering "the right kind of knowledge at the right time, to the right patient, at the right place"- a goal of personalized medicine. If we are to improve health outcomes, robust evidence must be generated and decision-making must be improved.
To accomplish these objectives, we must develop effective methods to measure the benefits and harms associated with our health care system and apply these methods within a rational and ethical framework. An integral aspect of this effort is to educate a new cadre of (clinical) researchers on rigorous (EBM, Patient-Centered) research methods. In addition, the Division of Evidence-based Medicine (EBM) proposed to apply rigorous EBM methodology to link research, practice and educational efforts in order to improve clinical & education outcomes at the Department of Internal Medicine across diverse settings (Morsani Clinics,TGH etc).
About our Division of Evidence Based Medicine
Mission: to help integrate research, practice and educational efforts in order to improve clinical & education outcomes at MCOM and its partner institutions by assisting with the development of evidence-based medicine in the effort to improve clinical decisions, policy-decisions and decisions aimed to improve health of populations.
Vision: to transform the nature of relationship between research, education and practice by promoting EBM standards leading to creating a culture where EBM decision-making, education and research will become an accepted norm and to become one of the national leaders in EBM research and education.
Goals:
- to strategically position the Division of EBM as a natural link between all Departments at MCOM, USF Health and its partners (such as CAMLS, Villages, TGH, etc.)
- to conduct scholarly & research activities in EBM;
- to help educate a new cadre of researchers in rigorous research methods; and
- to help promote and develop research and educational EBM techniques to connect data
generated in institutional clinical research, biomedical literature, and practice-based research networks.
This year the EBM team has generated more than 50 publications, and the Division Chief authored more than 25 papers in peer review journals. We are extraordinary proud by this year's publication in two top scientific journals. This is the first time USF faculty published two papers in these two journals.
Djulbegovic B, Kumar A, Glasziou P, Miladinovic B, Chalmers I. Trial unpredictability yields predictable therapy gains. Nature 2013;500:395-396 Scored top 5% of articles by attention
Bennett C, Djulbegovic B, Norris L, Armitage JO. Colony-Stimulating Factors for Febrile Neutropenia in the Cancer Setting. N Engl J Med 2013;368:1131-9.
This article defines medical standards in the field, and in turn influences practice patterns more than any other types of publication. Methodological papers of importance for the field of evidence-based medicine and decision-making
Djulbegovic B, Hozo I, Beckstead J, Tsalatsanis A, Pauker SG. Dual processing model of medical decision-making. BMC Medical Informatics and Decision Making.2012, 12:94.
This paper describes a novel model of medical decision-making and is selected by the Editorial Board of the 2013 IMIA (International Medical Informatics Association) Yearbook of Medical Informatics "for listing in the Yearbook as one of the best articles from the literature in medical informatics published in the past year"
Mann H, Djulbegovic B. Comparator bias: why comparisons must address genuine uncertainties. J R Soc Med 2013: 106:30-33
Helps doctors and researchers understand how to select best comparator and spot the design of the studies when inferior comparators in clinical studies were used
Ioannidis JPA, Hozo I, Djulbegovic B. Optimal type I and II error pairs when the available sample size is fixed. J Clin Epidem 2013; May 9. pii: S0895-4356(13)00088-7. doi: 10.1016/j.jclinepi.2013.03.002. [Epub ahead of print]
Considered as a major methodological breakthrough for studying rare diseases
Miladinovic B, Kumar A, Hozo I, Mhaskar R, Mahony H, and Djulbegovic B. Optimal information size in trial sequential analysis of time-to-event outcomes reveals potentially inconclusive results due to the risk of random error. Journal of Clinical Epidemiology 2013; PMID: 23403248
Important methodological advances for research synthesis field and design and interpretation of clinical research.
Veenstra DL, Piper M, Haddow JE, Pauker SG, Klein R, Richards CS, Tunis SR, Djulbegovic B, et al: Improving the efficiency and relevance of evidence-based recommendations in the era of whole-genome sequencing: an EGAPP methods update. Genet Med. 2013 Jan;15(1):14-24
This paper describes the state of art methods for developing studies for personalized medicine. It consists of the leading experts around the country in genomics and EBM and is run by CDC. It is a great privilege and honor to be invited to participate in this group.
Welcome Dr. Ben Djulbegovic and the EBM Team to the Department of Internal Medicine!
|
|
Patient-Centered Care: Putting Compassion into Practice
|
|
IM SUSTAINABLE: a Pallavi and Kiran Patel Project
 The Department of Internal Medicine is excited to launch the first of our international initiatives, working with the International Health Student Collaborative (IHSC) and the Patel College of Global Sustainability. The Department of Internal Medicine is excited to launch the first of our international initiatives, working with the International Health Student Collaborative (IHSC) and the Patel College of Global Sustainability.
Our program will utilize a cross-disciplinary global community approach to resolving medical issues in the United States and abroad. By embracing a more preventive evidenced-based approach to include clinical care blended with population-based and environmental science, we seek to develop lasting and sustainable solutions that complement the efforts of the Patel College of Global Sustainability and blend efforts with the College of Public Health and other members of USF Health.
This program will bridge sustainable development and clinical care internationally. To fulfill our medical college goals of clinical care, research and education we will be forming country-specific teams.
A needs assessment for the Panama program and India program is planned for completion around February 2014.
This Spring we will be sending a team to a developing country with the IHSC. To amplify this effort a grant from the Kiran and Pallavi Patel Family Trust will support the travel of:
- 1 student from the Patel College of Global Sustainability
- 1 or 2 faculty in Internal Medicine or Internal Medicine Peds
- 1 or 2 Internal Medicine trainees
- 2-3 medical students from Internal Medicine and International
Through this initiative, the Department of Internal Medicine and the Patel College of Global Sustainability will link to each others' web sites and demonstrate we are the clinical arm of the Kiran C. Patel College of Global Sustainability.
The selection committee for reviewing applicants will be:
- Cuc Mai, MD Residency Director
- John Sinnott, MD, FACP Chair, Internal Medicine
- Lynette Menezes, PhD Assistant Vice President, USF Health International
- Margarita Cancio, MD, FACP Founding Trustee, USF
- Dr. Kiran C. Patel, MD, FACP Cardiologist, Philanthropist
As part of the selection process, we will ask applicants to provide a 300 word personal statement explaining what they hope to gain/learn from the experience and how it will enhance their professional or personal growth. Applications will be due Nov 15th and notification of awards will take place January 15th.
|
We look forward to improving medicine globally with the Patels!
|
Have newsworthy content? Have questions about the DOIM? Help us get it acknowledged!
The DOIM has many ways of sharing our successes. Content to consider:
- Nominations for those who go above and beyond
- Faculty, Research, Resident or Fellow feature (including patient-centered focus)
- Accomplishments, Awards and Accolades
- Publications
- International Activities
- Socializing/Networking Opportunities
- Interesting articles you think the DOIM would benefit from
- Questions on policies, procedures or general inquiries
Please email submissions for consideration in all our marketing materials.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12901 Bruce B Downs Blvd MDC19, Tampa, FL 33613 � 813.974.4067
|
|
Copyright � 2013. All Rights Reserved.
|
|
|
|