|
|
Dilated Cardiomyopathy
and Associated Conditions
|
|
Age/Breed:
6-year-old MN
Giant Schnauzer
Referred by:
Dr. Clark at Western Branch Veterinary Hospital
|
|
|
By:
Merrilee T. Small, DVM, DACVIM (Cardiology)
History: 11/17/2016. Otis, a six-year-old, 57.7 kg MN Giant Schnauzer, presented to Western Branch Veterinary Hospital with a 2-3
day history of lethargy, dry cough and diarrhea. Otis was treated for heartworm disease at ~ 4 years of age, and an arrhythmia had been ausculted at routine physical exams since. He was fed
Diamond Naturals Lamb and Rice. A tachyarrhythmia with pulse deficits was ausculted on PE and he was promptly referred to The COVE's ER and Cardiology services. Otis was mentally dull/weak, tachycardic and arrhythmic on presentation. A gallop sound was present, most audible on the right. An electrocardiogram revealed atrial fibrillation with a ventricular response rate of 180-210 bpm. TFAST revealed mild pleural and trivial pericardial effusions and a subjectively hypocontractile heart. Labwork revealed creatinine 2.0 mg/dL (
0.5-1.8mg/dL), total T4 < 0.5 ug/dL (0.8-3.5), TSH 1.86 ng/mL (0.0-0.6) and free T4 6 pmol/L (8-40). A diagnosis of dilated cardiomyopathy with severe systolic dysfunction and global cardiac enlargement was confirmed
by The COVE's Cardiology Department. He was stabilized and the following medical therapies were instituted: pimobendan 15 mg PO TID, benazepril 30 mg PO q 24 hours, furosemide 120 mg PO TID, spironolactone 75 mg PO q 24 hours, diltiazem titrated from 15 mg TID to final dose of 90 mg PO TID based upon ECG monitoring, levothyroxine 0.3 mg PO BID, and fish oil supplement 1800 mg of the EPA component daily.
12/2016 - present: Otis' respiratory effort, cough, and exercise tolerance all improved following therapy. Ventricular response rate measured 150-160 on ECG, recorded at rechecks. As of this writing, Otis continues to enjoy a very high quality of life. His hypothyroidism is well controlled. He developed pleural effusion in September 2017 and is now on 160 mg furosemide PO TID and 50 mg hydrochlorothiazide PO BID in addition to his previous medications. A mild residual effusion is chronically present. Labwork is routinely monitored and he has a mild azotemia without electrolyte imbalance.
Discussion: Dilated cardiomyopathy (DCM) accounts for about 10% of cardiac disease in the dog. Males are affected more commonly than females. There are multiple causes of DCM in the dog. Doberman Pinschers, Boxers, Great Danes, English Cocker Spaniels and Giant breeds are predisposed to it, and genetics are likely the cause. A genetic link has been confirmed in Dobermans and Danes. Other potential causes include blood or myocardial taurine or L-carnitine deficiencies. Low plasma taurine levels have been documented in affected dogs on homemade, lamb/rice, and more recently some grain-free diets. Dietary history should be investigated in any atypical breed diagnosed with DCM. Myocarditis due to toxins or infectious disease is another potential cause of DCM. Endocrinopathies such as hypothyroidism and hypoadrenocorticism have been associated with systolic dysfunction. Pacing-induced cardiomyopathy occurs when a sustained heart rate of > 190-200 bpm (usually an arrhythmia) occurs over a period of several weeks. Alas, many cases of DCM are diagnosed as idiopathic.
Affected dogs often present with signs of left, right, or biventricular heart failure, a soft cough (common in deep-chested dogs), and syncope. Prognoses vary with etiology and breed. Dobermans and Danes tend to experience rapidly progressive clinical courses, with the prognosis often only 4-10 months even with aggressive treatment. Other patients may have much more time. Unfortunately, sudden cardiac death due to ventricular arrhythmia is a complication that could significantly reduce life expectancy.
Atrial fibrillation (AF) can be present in giant breed dogs without overt echocardiographic evidence of myocardial dysfunction. This is termed "lone atrial fibrillation." Most patients with lone AF develop systolic dysfunction or overt DCM over time. AF is more commonly associated with structural heart disease and occurs in ~ 45% of dogs with DCM. AF is typically permanent. Therefore, control of the ventricular response (VR) rate is targeted. The VR cannot be counted by auscultation alone, as not every electrical impulse will result in sufficient muscular contraction to generate a heart sound. ECG is necessary to document the VR. Optimal heart rate control (VR < 125 bpm on 24-hour Holter monitor at home) is positively associated with improved survival. The best rate control is achieved with a combination of diltiazem and digoxin. On ECGs performed in the hospital, a VR below 155 bpm appears to correspond to around 130 bpm at home. Optimized monitoring at home may be achieved with 24-hour Holter monitoring or through owner use of an Alivecor or Kardia veterinary monitor.
References available upon request.
|
|
|
TECH TIP:
Counting Atrial Fibrillation Heart Rates
By: Marie Moore, LVT and Andi Davis, LVT
|
|
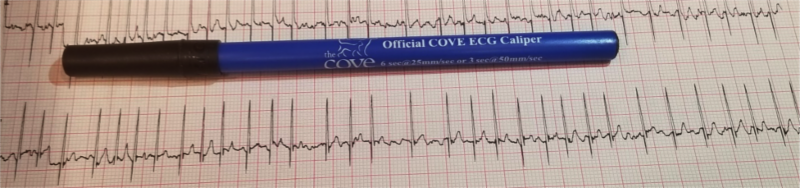
It is almost impossible to obtain a heart rate for patients in atrial fibrillation by auscultation alone. Here are two quick methods available to obtain heart rates from an ECG.
The Pen Method ("Pen Times Ten")
- A typical BIC pen equals 6 seconds with 25mm/sec paper speed.
- Count the QRS complexes to the end of the pen and multiply by 10 to obtain bpm.
Note: If paper speed is set at 50mm/sec, multiply count by 20 to obtain bpm.
|
|
QRS Complexes = 23 HR = 230bpm
|
The R-R Interval Method (Instantaneous Heart Rate)
- Identify two sequential R-waves and count the number of small boxes between waves
(Each square represents 0.04 seconds at 25mm/sec).
- Multiply the number of squares by 0.04 seconds to obtain beats/sec.
- Divide beats/sec by 60 (sec/min) to obtain bpm.
|
Instantaneous HR #1
# Squares = 6
Beats/sec = 0.24
HR = 250bpm
|
Instantaneous HR #2
# Squares = 11
Beats/sec = 0.44
HR = 136bpm
|
|
|
COVE News
|
|
COVE News
|
|
|
|
|
May 2018 marks our 6th anniversary!
===================
Join us at The COVE Seaside CE Event in Virginia Beach, May 27, 29, 30, and 31, 2018
Enjoy the salty air, let down your hair and join us for a complimentary continuing education event for doctors, technicians, and managers featuring topics in cardiology, surgery, critical care, and dentistry. Attend one or attend them all - a unique opportunity to earn up to 9 CE credits! Meals will be served.
To register, email: [email protected]
===================
Dr. Merrilee Small and Hospital Manager Danielle Russ will attend
ACVIM Forum
in Seattle June13-16. This year's theme, Innovation, Science + BEYOND is sure to be inspiring and educational. Let us know if you're going to be there! We'd love to see you.
|
The COVE offers Minimally Invasive Surgery (MIS)
In cases where surgery is required, we always look for options that will cause the least amount of pain and provide the quickest recovery option for our patients. In a minimally invasive procedure, small incisions are made and used as passageways for a
laparoscope
or
endoscope
, which are tiny fiber optic video cameras. Working from the images provided from the scope, special instruments are then passed through other openings and operated by remote control to perform the necessary procedure.
Benefits to your patients:
- Smaller incisions
- Quicker recovery time
- Less pain
- Less scarring
- Lower risk of infection
- Reduced blood loss
We offer MIS for:
- Laparoscopy: Abdominal and pelvic surgery
- Thoracoscopy:
Lung/chest surgery
- Arthroscopy: Joint surgery
Would you like to learn more?
Please call us anytime!
|
As part of our dedication to the veterinarian community, we offer a variety of CE opportunities for DVMs, LVTs, and support staff.
Our Lunch and Learns are complimentary educational sessions at your practice during your lunchtime.
Presentations are given by a COVE team member and are approximately 30 minutes to 1 hour in length. You choose the topic and we'll bring the education and food to you!
Some of our most common Lunch and Learn topics are:
- Anesthesia & Analgesia
- Bandaging/Splinting
- CPR
- Dental Emergencies
- ECG Review
- Echocardiography
- ER Triage
- Hypertension
- History and Physical Examination
- Radiographs (dental, thoracic and/or orthopedic)
If you don't see a topic of interest, let us know what you would like to learn about. We'll do our best to accommodate.
To schedule a Lunch and Learn, please contact Danielle Russ, Hospital Manager, with your preferred topic and date
at
[email protected] or 757.935.9111.
|
|
|
24/7 Emergency and Critical Care | Surgery | Cardiology | Dentistry
|
6550 Hampton Roads Pkwy, #113 | Suffolk, VA 23435
P: 757.935.9111 | F: 757.935.9110 |
thecovevets.com
|
 |
|
|
|
|
|
|