December:
Management of Acute and Chronic Nasal Fracture
January 2014:
Pediatric Amplification
February 2014:
In-Office Treatment of Radiation Fibrosis of True Vocal Folds
|
Our E-Update Newsletters are designed to provide brief, practical, clinical updates in areas where we all struggle in managing our patients. To view past issues, please visit our Archives. |
February 2014
Charleston Sleep Surgery Symposium
March 2014
Pediatric ENT Update
Pediatric Audiology Conference
April 2014
Temporal Bone Dissection Course
May 2014
Sinus Masters
Southern States Rhinology Course Charleston Magnolia Conference
July 2014
The Charleston Course: Otolaryngology Literature Update
For program brochure, registration form, and more, please visit
our website.
|
We want to hear from you!
We welcome your feedback - answers, questions, input - on our newsletter articles as well as any ENT questions you may have. If there are topics you are interested in learning more about, please
|
|
|
In our November ENT E-Update, M. Boyd Gillespie, M.D., M.Sc., Director, MUSC Snoring Clinic, describes upper airway stimulation therapy as an alternative surgical approach to treat obstructive sleep apnea.
Hypoglossal nerve stimulation will be one of the many topics covered in Dr. Gillespie's 3rd Annual Charleston Sleep Surgery Symposium and will include a live patient interview. This well-attended course to be held February 21-22, 2014 for practicing otolaryngologists offers lectures and hands-on labs focused on procedures for snoring and sleep disordered breathing. Be sure to reserve your seat early, especially for the lab as it fills up quickly!
More information on Dr. Gillespie follows the article below and is on our website.
Please feel free to contact us with feedback or questions about the E-Udate articles, your patients, or any other ENT issue at [email protected].
Paul R. Lambert, MD
Professor and Chair
|
|
 | |
Dr. M. Boyd Gillespie, Director, MUSC Snoring Clinic
Medical University of South Carolina
|
Hypoglossal Nerve Stimulation for Obstructive Sleep Apnea
| |
Obstructive sleep apnea (OSA) is a highly prevalent disorder contributing to significant medical morbidity, sleep disturbance, impaired quality of life, and an increased risk of motor vehicle accidents. Moderate or severe disease may affect greater than 7% of the adult population.1 It results from the interaction of an anatomically smaller and more vulnerable upper airway, loss of physiologic compensation, and reduced upper airway muscle dilation during sleep. Currently, the first line therapy for moderate to severe OSA is the use of positive airway pressure which acts as an upper airway stent to maintain the patency of the upper airway during sleep. Nasal CPAP (continuous positive airway pressure) demonstrates high efficacy in treating OSA. However, the effectiveness of CPAP is limited by poor patient acceptance with long-term adherence rates of only 50-70%.2 As a result, alternative therapies are required as salvage treatment for many individuals with symptomatic OSA who fail CPAP therapy.
One historical alternative to treat OSA is surgery. Surgical procedures either bypass the obstructed upper airway or attempt to reduce the structural vulnerability of the upper airway. Tracheotomy bypasses the upper airway for patients with life-threatening OSA, however long-term tracheotomy-related morbidity make it unacceptable for most routine cases of OSA. In contrast multiple surgical procedures have been developed that modify soft tissues surrounding the pharynx either by tissue reduction (ex. tonsillectomy, UPPP, partial glossectomy) or tissue stabilization and advancement (ex. maxillomandibular advancement, genioglossal advancement, hyoid suspension, tongue suspension). Acceptance is variable due to side effects and lack of high quality data on effectiveness for many procedures. 3 An alternative surgical approach to treat OSA is therefore desired. Electrical stimulation of the hypoglossal nerve has been proposed as a physiologic method to maintain upper airway patency. Whereas traditional surgical approaches irreversibly alter the tissue of the upper airway, hypoglossal nerve stimulation augments tone to the upper airway to maintain airway patency. Pre-clinical studies found that stimulation of the hypoglossal nerve reduced upper airway collapsibility in an animal model. 4 Early feasibility studies in humans showed that stimulation could increase maximal inspiratory airflow during sleep by 100% without causing an awakening. 5 An initial phase I trial of a first-generation device in 8 patients showed a significant decrease in the apnea-hypopnea index (AHI), however the device was prone to malfunction over time. 6 A recent phase II trial of a second generation device (Upper Airway Stimulation (UAS) system, Inspire Medical Systems, Minneapolis, MN, USA) demonstrated a high-rate of physiologic resolution of apnea (78% of patients with a 50% reduction in AHI and overall AHI<20) with significant improvements in daytime sleepiness and sleep-related quality of life in successfully treated patients. 7 Activation of the device during sleep prevents pharyngeal collapse and maintains airway patency throughout the respiratory cycle ( Figure). 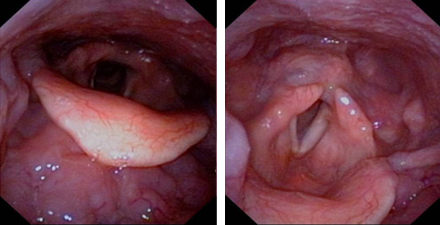 | |
Figure: A collapsed hypopharyngeal airway (left) opens with stimulation of the hypoglossal nerve (right).
|
A large scale phase III study (STAR Trial, Inspire Medical Systems, Minneapolis, MN, USA ) of 124 patients completed in early 2013 demonstrated promising results and will be published in the medical literature soon. Five of the six patients (83%) surgically implanted at MUSC were considered a success and continue to use the device on a regular basis. The device is currently under consideration of approval with the FDA, and may be available to the public as a viable option for moderate-to-severe obstructive sleep apnea in CPAP failures as early as 2014.
M. Boyd Gillespie, M.D.
Associate Professor; Director, MUSC Snoring Clinic
Medical University of South Carolina
|
REFERENCES:
1. Young T, Palta M, Dempsey J, Peppard PE, Nieto FJ, Hla KM. Burden of sleep apnea: rationale, design, and major findings of the Wisconsin Sleep Cohort study. WMJ. 2009;108(5):246-9.
2. Richard W, Venker J, den Herder C, et al. Acceptance and long-term compliance of nCPAP in obstructive sleep apnea. Eur Arch Otorhinolaryngol. 2007; 264: 1081-86.
3. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modification of the upper airway for obstructive sleep apnea in adults: a systematic review and meta-analysis. Sleep 2010; 33: 1396-407.
4. Smith PL, Eisele DW, Podszus T, et al. Electrical stimulation of the upper airway musculature. Sleep 1996; 19 (10 Suppl.): S 284-7.
5. Schwartz AR, Eisele DW, Hari A, et al. Electrical stimulation of the lingual musculature in obstructive sleep apnea. J Appl Physiol. 1996; 81: 643-52.
6. Schwartz AR, Bennett ML, Smith PL, et al. Therapeutic electrical stimulation of the hypoglossal nerve in obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 2001; 127: 1216-23.
7. Van de Heyning PH, Badr MS, Baskin JZ, et al. Implanted upper airway stimulation device for obstructive sleep apnea. Laryngoscope 2012; 122: 1626-33.
|
About Dr. Gillespie...

M. Boyd Gillespie , M.D.
- Associate Professor
- Director, MUSC Snoring Clinic
Residency: Johns Hopkins
Fellowship: Johns Hopkins
Special interest: Laryngology, swallowing disorders, sleep apnea, head and
neck tumors.
|
|
|
|
|

