January 2014:
Pediatric Amplification
February 2014:
In-Office Treatment of Radiation Fibrosis of True Vocal Folds March 2014:
Surgery for Hyperparathyroidism
|
Our E-Update Newsletters are designed to provide brief, practical, clinical updates in areas where we all struggle in managing our patients. To view past issues, please visit our Archives. |
February 2014
Charleston Sleep Surgery Symposium
March 2014
Pediatric ENT Update
Pediatric Audiology Conference
April 2014
Temporal Bone Dissection Course
May 2014
Sinus Masters
Southern States Rhinology Course Charleston Magnolia Conference
July 2014
The Charleston Course: Otolaryngology Literature Update
For program brochure, registration form, and more, please visit
our website.
|
We want to hear from you!
We welcome your feedback - answers, questions, input - on our newsletter articles as well as any ENT questions you may have. If there are topics you are interested in learning more about, please
|
|
|
In our final ENT E-Update of 2013, Judith M. Skoner, M.D., describes management of adult acute nasal fractures - critical factors to note in diagnosis, types of nasal fractures, timing of treatment, and treatment decisions for optimizing outcomes.
More information on Dr. Skoner follows the article below and is on our website. Please feel free to contact us with feedback or questions about the E-Udate articles, your patients, or any other ENT issue at [email protected].
We appreciate your continued support throughout the year. May you and your families be blessed with a safe and joyous holiday season!
Paul R. Lambert, MD
Professor and Chair
|
|
 | |
Judith M. Skoner, M.D. with mentor, Mark K. Wax, M.D., Professor, Director, Microvascular Reconstruction, Oregon Health and Science University.
|
Management of Adult Acute Nasal Fractures
| |
The most common type of facial fracture is the nasal bone fracture, with motor vehicle accidents, sports injuries, falls and physical altercations as the most frequent causes 1, 2. Despite the frequency of nasal fractures, the treatment of acute nasal bone trauma remains controversial.
The diagnosis of isolated nasal fractures is primarily based on a thorough history and physical examination, although plain radiographs and CT scans are frequently obtained prior to presentation to a specialist. A preliminary study recently reported ultrasound for detecting nasal fractures in adults as a radiation-free alternative to diagnostic imaging 3. Ultimately, however, treatment decisions for the acute adult nasal fracture are still based heavily on physical exam and clinical judgment. Critical factors to note and address immediately upon presentation include mechanism of injury, timing of event, pre-injury status and prior trauma/surgery, patient expectations and goals, intranasal drug use, paresthesias, nasal airway obstruction, csf rhinorrhea, intracranial/orbital injury, other facial fractures, soft tissue trauma and septal hematoma.
Timing of treatment for acute nasal fractures varies, but reports suggest optimal treatment between 3 and 30 days 2,4. This writer prefers to treat the isolated acute adult nasal fracture either within the first few hours post-event before the edema becomes too confounding, or between post-injury days 3 to 14, to allow for decreased edema and a more accurate clinical assessment of the deformity.
Classifications of nasal fracture types have been proposed by multiple sources, with the goal of providing a framework to guide repair 5,6,7. A general theme to most, however, is a more conservative approach to simple nasal fracture repair, with consideration of more invasive repairs dedicated to more extensive fractures. A nasal fracture classification based on symmetry, septum status and overall injury severity, describes Type I injury as the most simple straight fracture, and progresses to Type V injury as the very complex nasoseptal trauma, including soft tissue injury with open compound fractures 8. That same group of authors concluded that patients in their study had similar outcomes via open or closed treatment of acute nasal fractures-- if the surgical approach was well-matched to the individual fracture 8. Thus, as is true for other facial reconstructions, the management of acute nasal fractures should take into consideration the specific fracture characteristics, as well as individualized patient factors.
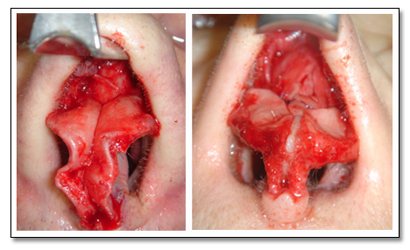 | |
Figure 1: Warped medial crura s/p prior nasal-septal fractures, exposed for repair at time of secondary open septorhinoplasty for chronic nasal deformity
Figure 2: Columellar/caudal strut and dome sutures placed along with spreader grafts at time of secondary open septorhinoplasty for chronic nasal obstruction after prior nasoseptal fractures
|
Closed reduction of isolated nasal fractures has long been described in the acute setting with no incisions, low morbidity and reported success rates of 60-90% 9. A systematic review showed no difference in outcomes functionally or aesthetically after closed reduction using local anesthesia versus general anesthesia, so this technique may be performed in the office setting with cooperative patients 10. External injection of local anesthetic and/or topical applications were studied as well in that report, and the least painful method of local anesthetic was tetracaine gel applied to the nasal dorsum, in combination with topical intranasal cocaine solution 10. For the reduction itself, the skull base is protected and nasal elevators are used in association with digital manipulation to realign the fracture segments; the Asch forceps are particularly helpful with septal fracture reductions. Once the surgeon and patient are satisfied with the reduction, external splinting is routinely performed by this writer for 7-10 days post-reduction; intranasal silastic splinting is typically reserved for septal fractures, intranasal lacerations and severely comminuted depressed nasal bone fractures.
Despite the study cited earlier 8, prior reports note that up to 50% of acute closed nasal fracture reductions may result in post-procedure deformities necessitating secondary septoplasty or septorhinoplasty 11. For this reason, some authors advocate more aggressive open reductions, or formal septorhinoplasty, in the acute setting 7,9,11, rather than delaying open interventions 6+ months post-injury, as per the more traditional approach. Ondik and Fedok et al 8 describe their approach using both open and closed reduction philosophies in the acute setting, with a 'modified open repair'. This technique is essentially a closed reduction with the addition of endonasal stab incisions for completion osteotomies in patients with impacted or greenstick/displaced fractures not otherwise well-reduced. The concept of employing multiple techniques in a stepwise fashion, individualized to specific fracture characteristics, may be key to optimizing outcomes in complex fracture management 6,9.
Many surgeons, including this writer, maintain that closed reduction (+/- individualized modification when appropriate) is the mainstay of acute isolated nasal fracture treatment in adults, with more aggressive open approaches reserved for severe nasal and septal fractures, and those associated with other facial, orbital or cranial fractures 8. Formal septorhinoplasty may be performed approximately 6-9 months after closed reduction if needed, in cases with persistent nasal obstruction and/or deformity. It is crucial in these secondary approaches to chronic nasal fractures and the crooked nose, to not only address the aesthetic deformity, but to adequately address the structural nasal airway support and enhance this. In such cases, this writer finds spreader grafts - often intentionally asymmetric to help correct c-deformities-- and other supportive grafting and suture techniques exceptionally useful in maximizing nasal form and function in the secondary septorhinoplasty.
Judith M. Skoner, M.D.
Medical University of South Carolina
|
REFERENCES:
Renner GJ. Management of nasal fractures. Otolaryngol Clin North Am. 1991;24(1):195-213.
2. Fernandez SV. Nasal fractures: The taming of the shrewd. Laryngoscope. 2004;114:587-592.
3. Ardeshirpour F, Ladner KM, Shores CG, Shockley WW. A preliminary study of the use of ultrasound in defining nasal fractures: Criteria for a confident diagnosis. Ear, Nose & Throat Journal. 2013;92(10-11):508-512.
4. Chan J, Most SP. Diagnosis and management of nasal fractures. Op Techniques in Otolaryngol. 2008;19:263-266.
5. Stranc MF, Roberson GA. A classification of injuries of the nasal skeleton. Ann Plast Surg. 1979;2:468-474.
6. Murray JA, Maran AG, Busuttil A, Vaughan G. A pathological classification of nasal fractures. Injury. 1986;17:338-344.
7. Higuera S, Lee EI, Cole P, Hollier LH Jr, Stal S. Nasal trauma and the deviated nose. Plast Reconstr Surg. 2007;120(7, Suppl 2):64S-75S.
8. Ondik MP, Lipinski L, Dezfoli S, Fedok F. The treatment of nasal fractures: A changing paradigm. Arch Facial Plast Surg. 2009;11(5):296-302.
9. Staffel JG. Optimizing treatment of nasal fractures. Laryngoscope. 2002;112:1709-1719.
10. Chadha NK, Repanos C, Carswell AJ. Local anaesthesia for manipulation of nasal fractures: systematic review. J Laryngol & Otology. 2009;123:830-836.
11. Rohrich RJ, Adams WP Jr. Nasal fracture management: minimizing secondary nasal deformities. Plast Reconstr Surg. 2000;106:266-273.
|
About Dr. Skoner...

Judith M. Skoner , M.D.
- Assistant Professor
M.D.: University of South Carolina
School of Medicine
Residency: MUSC
Fellowship: Oregon Health and
Science University
Special interest:
Microvascular reconstructive surgery of the face/head & neck, facial reanimation for facial paralysis, facial/nasal trauma management and reconstruction, and Mohs defect reconstruction.
|
|
|
|
|

