|
The old medical school mnemonic "bones, stones, groans, and psychiatric overtones" still well describes the symptoms experienced by patients with primary hyperparathyroidism. These include skeletal complications (pathologic fractures, osteitis fibrosa cystic, osteoporosis), renal disease (nephrolithiasis, nephrocalcinosis, diabetes insipidus, renal failure), gastrointestinal symptoms (constipation, nausea, vomiting), psychiatric symptoms (mood swings, depression, psychosis) and central nervous system complaints (lethargy, ataxia, delirium). However, many patients present only with signs of elevated serum calcium and parathyroid hormone (PTH) levels and subtle symptoms of fatigue, depression, emotional lability, joint pain, or abdominal pain.
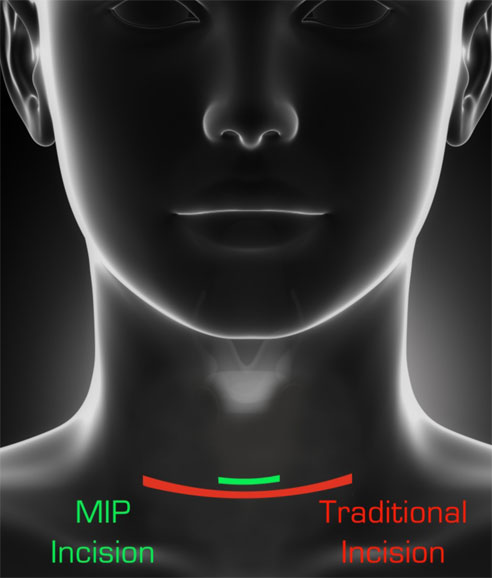
There is no definitive medical treatment for primary hyperparathyroidism, but there is a cure possible with surgery - a procedure called a parathyroidectomy. In the past, parathyroidectomy involved an open procedure with a neck incision not unlike that used for a thyroidectomy, and it required the inspection of all four parathyroid glands, with removal of the offending gland or glands. However, with improvements in diagnostic and surgical techniques, there has been a push toward less invasive procedures, with a goal of decreased recovery time, increased cosmesis, and decreased operative time and complications.
Minimally Invasive Parathyroidectomy (MIP), therefore, has become the preferred method of operation for the parathyroid glands. In this procedure, patients who are a candidate for surgery undergo a localizing scan to pinpoint where the abnormal gland is. This is usually done with a sestamibi scan or ultrasound (or sometimes both). When the gland is localized, a small incision can be made and the diseased gland removed without the need to disturb the unaffected glands. This results in shorter surgeries, less recovery and fewer complications.
There are several advantages to MIP. First, by operating only on one very small area of the neck - as opposed to dissecting all of the neck structures - the average operative time is less than 40 minutes, which can be compared to the standard parathyroid surgery that takes two to three hours or more. In addition, almost all patients are sent home within an hour or two of the operation compared to a standard operation which often leads to a 1-2 day hospital stay. Also, because the operative area is smaller there is less pain and quicker recovery. Lastly, and perhaps most importantly, the reported outcomes from MIP are between 95-100% with complication rates less than half those of the standard parathyroidectomy.
Within the Department of Otolaryngology-Head and Neck Surgery at the Medical University of South Carolina, we have several physicians adept at minimally invasive parathyroidectomy techniques.
|
Advantages of Minimally Invasive Parathyroidectomy
- Less anesthesia
- Smaller incision
- Less pain
- Short operating time
- No risk to nerves & other structures on the normal side of the neck
- The complication rate is significantly less when compared to the standard operation
- Significantly less expensive than the standard surgery
- Return to normal activities early (usually by the next day)
- Patient will almost always get to go home the same day
|
|
Eric J. Lentsch , M.D.
Medical University of South Carolina
|



