August: Contemporary Management of Infants with Pierre Robin Sequence
September:
Head and Neck Oncology
October:
Environmental Control Measures for House Dust Mite Allergy. What is the Evidence?
|
July 2013
The Charleston Course: Otolaryngolgy Literature Update
October 2013
Charleston Swallowing Conference
Head & Neck Oncology Sea to Summit
February 2014
Charleston Sleep Surgery Symposium
March 2014
Pediatric ENT Update
Sinus Masters
April 2014
Temporal Bone Dissection Course
May 2014
Southern States Rhinology Course Charleston Magnolia Conference
July 2014
The Charleston Course: Otolaryngology Literature Update
For program brochure, registration form, and more, please visit
our website.
|
We want to hear from you!
We welcome your feedback - answers, questions, input - on our newsletter articles as well as any ENT questions you may have. If there are topics you are interested in learning more about, please email us.
|
|
|
Dear Colleague,
In this ENT E-Update issue, I will describe options for treating single-sided severe to profound SNHL. I hope you find this information useful in your practice.
We will be hosting The Charleston Course, our 3rd Annual Otolaryngology Literature Update conference at the Kiawah Island Golf Resort July 26 - 28, 2013. In these three days, more than 100 select manuscripts will be reviewed, and those "pearls" important to your practice will be emphasized. I believe that there may be no better way to stay current in our field than with this Literature Update Course. I hope you will join us this July.
Please feel free to contact us with your feedback or questions about our E-Udate articles, your patients, or any other ENT issue at [email protected].
Paul R. Lambert, MD
Professor and Chair
|
|
 | |
Paul R. Lambert, M.D., Professor & Department Chair,
Director, Otology & Neurotology
|
Treatment of Single Sided Deafness
| Treatment of single sided severe to profound SNHL can be
accomplished with a variety of implants and prostheses, including:
- Bone anchored hearing aid
- Intraoral prosthesis
- CROS hearing aid
- Deep in the canal hearing aid
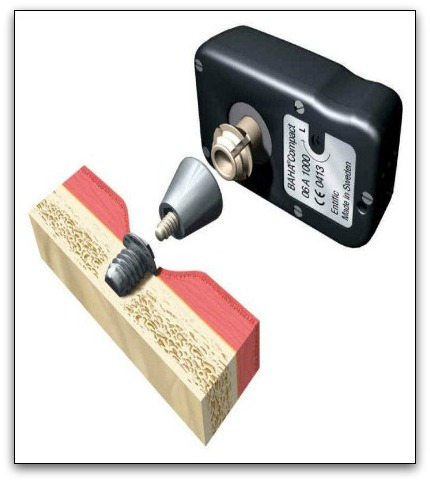
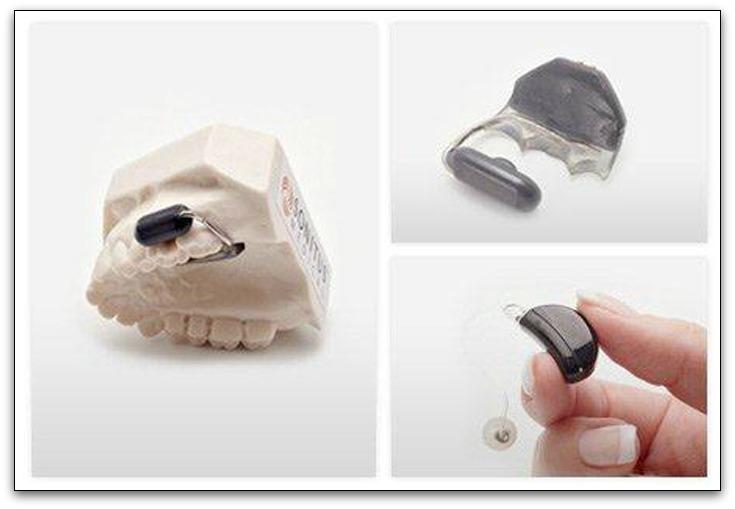
There are currently 3 implantable bone anchored systems: the Baha (Cochlear America), Figure 1; the Ponto (Oticon Medical), Figure 2; and the Sophono (Sophono Inc.), Figure 3. In each case, the implant is anchored to the bone behind the ear. Both the Baha and the Ponto require osteointegration of a transcutaneous abutment to which the external processor is attached. The Sophono, originally developed in Germany and now produced in Colorado, involves 2 hermetically sealed magnets in a titanium case that is placed completely beneath the skin and secured to the bone with maxillofacial screws. The external processor couples magnetically to the implant. All 3 bone conduction devices have been approved for patients older than 5 years. For children less than 5, a bone conduction device attached to a headband or "soft band" can be utilized.
 | | Figure 1. The Baha (Cochlear America) |
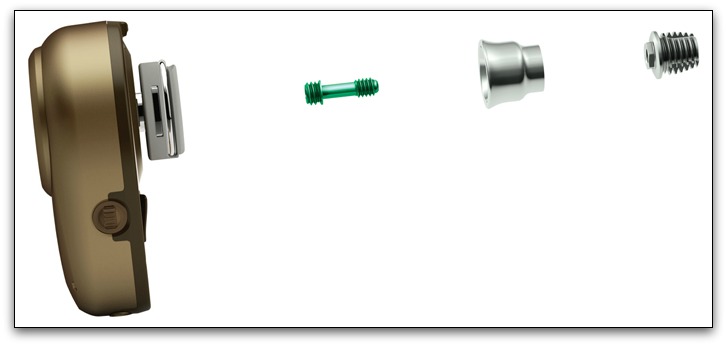 | | Figure 2. The Ponto (Oticon Medical) |
 | | Figure 3. The Sophono (Sophono, Inc.) |
It is anticipated that in the future a cochlear implant for single sided deafness will provide a superior solution to this problem.
The 3 preceding devices all require a short surgical procedure. Nonsurgical options include the intraoral prosthesis, SoundBite (Sonitous Medical), Figure 4, which uses the teeth to conduct the sound transcranially. With this device, a microphone is placed in the deaf ear and transmits the acoustic signal to the intraoral prosthesis which is attached to the molar teeth. A small piezoelectric actuator converts this acoustic signal to minute vibrations of the teeth and then on to the contralateral cochlea. The deep in the ear hearing aid (TransEar, Ear Technology Corporation) interfaces with the bone of the external auditory canal to initiate the transcranial sound transmission. Finally, the traditional CROS (contra-routing of signal) hearing aid system simply sends the signal by radiofrequency from the microphone/transmitter on the deaf ear to the receiver on the intact ear.
 | | Figure 4. SoundBite (Sonitous Medical) |
It should be noted that there is a slight (average 10 dB) attenuation of sound transmitted trans-cranially via bone conduction. Therefore, the recipient of a bone conduction device should have hearing thresholds across the speech frequencies in the good ear of 20-25 dB or better for optimal benefit. The BICROS hearing aid would be ideal for those individuals with greater than a mild hearing loss in the good ear. In this situation, the receiver in the good ear incorporates an amplifier to overcome the hearing loss.
Each of the systems discussed above have advantages and disadvantages. Transcutaneous abutments (Baha and Ponto) occasionally develop minor infection around the implant site. On the other hand, they most efficiently couple the signal to the bone. The Sophono is attractive because there is no transcutaneous component, thus eliminating the possibility of infection. Because of the magnetic transcutaneous coupling, however, there is a very slight loss of signal power. The SoundBite is attractive because it requires no surgery and is removable. A dentist must be involved, however, and insurance coverage may require more effort. A deep in the canal hearing aid concept is attractive cosmetically, but comfort and efficiency are the issues. The CROS hearing aid is a nonsurgical option, but it requires bilateral devices to be worn, with some patients objecting to a "hearing aid" in the good ear. As noted previously, if more than a mild hearing loss exists in the intact ear, the BICROS system is an excellent option.
Although sound localization is not possible with any of these devices, hearing in background noise is improved since the "head shadow effect" is eliminated. The shadow of the head attenuates sounds, particularly high frequency ones, from reaching the opposite side. Low frequency (long wavelength) sounds can "bend" around the head and reach the contralateral, intact ear. The high frequency (short wavelength) sounds, such as constanants, tend to be reflected by the head and are therefore less audible and clear. The head shadow effect is less a problem in face to face, one on one conversations. Talking primarily into the deaf ear (i.e., driver of a car with a right single sided deafness attempting to listen to a passenger) is more difficult. In a crowded environment a listener must hear conversation(s) from multiple spatial locations, and thus the head shadow effect becomes even more problematic. All the devices listed above ameliorate this problem to some degree.
Insurance companies have generally paid for the implantable bone conduction systems. Insurance coverage for the SoundBite may be more difficult, and coverage for a CROS or deep in the ear canal hearing aid are generally not covered by most insurance plans.
Professor & Department Chair,
Director, Otology & Neurotology
Medical University of South Carolina
|
About Dr. Lambert...

Paul R. Lambert, M.D.
- Professor
- Director, Otology & Neurotology
- Chair, Department of Otolaryngology
M.D.: Duke University
Residency: UCLA Hospital
Fellowship: Otologic Medical Group and House Ear Institute, Los Angeles
Special interests: Pediatric & adult ear diseases, hearing loss & tinnitus, vestibular diseases, chronic ear diseases
|
|
|
|
|

