|
|
ACPA UPDATE
APRIL/MAY 2025
|
| |
ACPA Membership Discount –
Expires May 14, 2025!
| | | |
NPAC 2025 in Chicago: Physician Advisors Reach New Heights | |
Stephanie Van Zandt, MD, ACPA-C
Medical Director Physician Advisor Services
Utilization Management/Complex Managed Care Denials
| | |
|
From April 7 to 10, 2025, the American College of Physician Advisors (ACPA) hosted its highly anticipated National Physician Advisor Conference (NPAC 2025) at the Chicago Marriott Downtown Magnificent Mile. With the theme “Healthcare Heroes: Physician Advisors Reaching New Heights,” the event attracted hundreds of physician advisors, healthcare executives, and industry leaders to the heart of Chicago, underscoring the expanding influence and critical role of physician advisors in today’s healthcare landscape.
Dynamic Agenda and Prestigious Speakers
NPAC 2025 delivered a robust three-and-a-half-day agenda, blending foundational education with advanced, forward-thinking sessions. The conference catered to both new and experienced physician advisors, featuring a separate course, “Essentials and Fundamentals” for those seeking certification and a strong grounding in core concepts. Attendees could earn up to 47.5 CME Category 1 credits, making NPAC 2025 one of the most comprehensive and cost-effective educational events in the field.
A major highlight was the keynote address by Dr. Christopher Windham, who spoke on Population Health and the evolving importance of physician advisors in driving system-wide improvements. Dr. Windham’s insights on integrating physician advisory roles into broader population health strategies resonated with attendees, emphasizing the need for adaptability and leadership as the healthcare environment continues to change.
ACPA President Dr. Clarissa Barnes delivered a compelling address, reflecting on the organization’s recent successes and outlining a vision for the future. Dr. Barnes stressed that the need for strong physician advisor leadership is greater than ever, given the rapid pace of change in healthcare policy, compliance, and patient care delivery.
Conference favorites such as the Observation Quiz Bowl and the Leadership Panel returned, offering lively, interactive opportunities for learning and engagement. The inaugural poster session was introduced at this year’s NPAC and was a resounding success showcasing intriguing and innovative projects by several physician advisors.
Recognition of Excellence and Leadership
NPAC 2025 was also a celebration of the profession’s leaders and innovators. The conference honored 13 ACPA Emeritus Physician Advisors, including the induction of two new members: Drs. Al Gore and Erica Remer. This recognition highlighted their longstanding dedication, mentorship, and impact on the physician advisor community.
Special awards were presented to acknowledge exceptional service and achievement. The Ronald Rejzer Distinguished Achievement Award, one of the highest honors in the field, was awarded to Dr. Dan Zirkman for his outstanding contributions to the ACPA. Additionally, the ACPA Distinguished Service Award recognized Drs. Ronald Hirsch and Erica Remer for their exemplary leadership and commitment to advancing the mission of the ACPA.
Networking, Collaboration, and Chicago’s Vibrant Setting
Networking remained a cornerstone of NPAC 2025, with a bustling exhibit hall and both small and large-scale events for attendees to connect, share best practices, and build lasting professional relationships. The Magnificent Mile location allowed participants to experience Chicago’s renowned museums, deep-dish pizza, and stunning skyline, further enhancing the conference experience.
Looking Ahead
NPAC 2025 set a new standard for professional development, celebrating the vital contributions of physician advisors as “healthcare heroes.” As the conference closed, excitement built for next year’s event, announced as a surprise on the final day: NPAC 2026 will take place in Charlotte, NC, April 14-16, with the theme “Revving Up for Success: Physician Advisors Driving Healthcare Forward”.
See you in Charlotte!
|
| | |
The Center for Successful Aging: Subacute at Home Program | A Collaboration to Expand Home Health Services | |
Bernie Ravitz, MD, FABQAURPABAM, PAC-CDI
Member, ACPA Observation Committee
| | |
|
The Center for Successful Aging at MedStar Health Good Samaritan Hospital and MedStar Health Home Care have partnered to create the Subacute at Home (“SaH”) program. This initiative addresses disparities and gaps in elder care in Baltimore City, Maryland. The program focuses on the most vulnerable older adults, often in underserved communities, by providing an intensive 30-day post-acute hospital rehabilitation, nursing, and medical treatment plan as an alternative to placement in a skilled nursing facility.
The program was first conceptualized out of delays in post-acute bed availability, particularly at skilled nursing facilities. MedStar was struggling to place patients out of the hospital and thus impacting the ability to care for patients requiring medically necessary hospital services. Conceptualized from a multidisciplinary team with the understanding that the SNF situation was likely not going to improve due to continued staffing challenges, they decided to come up with an alternative. In the discovery phase of this project, the team learned that the necessity of SNF often arose out of the lack of services in the home. The program was developed to fill this gap with the objective of creating Subacute at Home. The specific objectives included:
- Providing safe, high-quality medical care in the comfort of patients' homes.
- Helping patients recover, build strength, and regain independence while surrounded by loved ones.
- Educating patients and their caregivers on managing complex health conditions.
- Improving the patient and family experience.
- Bridging gaps in elder care coordination.
- Decreasing the total cost of care by reducing hospital length of stay, readmissions, and potentially avoidable emergency department visits.
Subacute at Home began in July 2023 and was fully operational by September 2023 as a MedStar Health Good Samaritan Hospital pilot program. The program is credited to the financial support from The Arthur E. Landers and Hilda C. Landers Charitable Trust who partnered with the MedStar Good Samaritan Hospital’s Center for Successful Aging. It has recently expanded to MedStar Health Union Memorial Hospital, with plans to extend to other MedStar Health Baltimore hospitals in early FY 25.
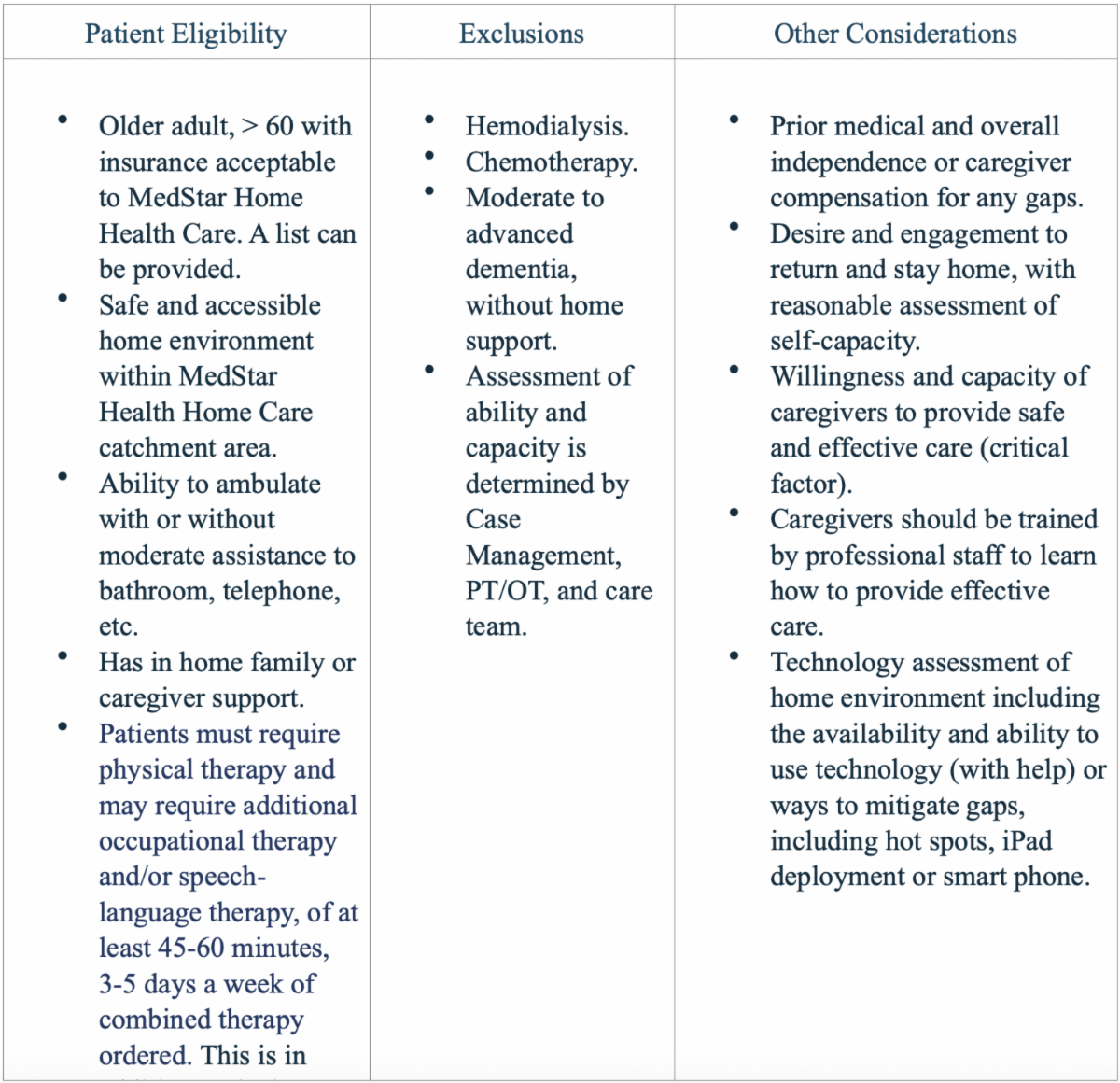
The program is a concentrated 30-day program available only to adults 60 years of age and older who meet specific criteria (see chart below). Patients are screened with the support of case management who evaluate the patients current home situation, caregiver supports, and potential needs once admission. When enrolled, patients receive home visits from experienced geriatricians and geriatric nurse practitioners (in-home and/or via telehealth), as well as traditional in-home healthcare visits (physical therapy, occupational therapy, speech-language pathology) at a higher frequency with more intense visits. Additionally, patients receive ongoing support for social determinants of health factors (e.g., partnership with Meals on Wheels), pharmacist consultations, and have home care aides assist with personal and respite care. At the end of the program, patients are smoothly and efficiently transitioned back to their primary care providers. If a patient does not have a primary care provider, a MedStar Health geriatrician will be recommended.
Patient Criteria
| |
Subacute at Home collaborates with the MedStar Health Research Institute’s Center for Biostatistics, Informatics, and Data Science to gather data, build a dashboard, and analyze outcomes to demonstrate the program's success. Data points include patient demographics, patient satisfaction, hospital length of stay, readmissions, the percentage of patients who remain home for three, six, nine, and twelve months, and the total cost of care. Current outcomes show that 32 patients have been admitted to the program, with one patient requiring hospice care. The transition to hospice care was smooth, thanks to an established relationship with Gilchrist Hospice Care.
The program continues to strive in success for keeping more patients at home. The care team has learned through this process that ongoing leadership collaboration and weekly patient huddles have been key to monitoring and ensuring success of the program.
The Subacute at Home program by the Center for Successful Aging at MedStar Health exemplifies a progressive approach to elder care, addressing critical gaps and providing an invaluable alternative to traditional skilled nursing facilities. By leveraging multidisciplinary collaboration and focusing on patient-centric care, the initiative has shown promising results in enhancing the quality of life for older adults, reducing hospital readmissions, and cutting overall healthcare costs. The continued success and planned expansion of the program demonstrates its effectiveness and the potential to optimize home services for the elderly. Looking ahead, the ongoing commitment to innovation and compassionate care is pivotal to overcoming the skilled nursing bed staffing and admission challenges.
References
- Augustine, M. R., Davenport, C., Ornstein, K. A., Cuan, M., Saenger, P., Lubetsky, S., Federman, A. D., DE Cherrie, L. V., Leff, B., & Siu, A. L. (Year). Implementation of Post-Acute Rehabilitation at Home: A Skilled Nursing Facility-Substitutive Model. Journal Name, Issue, Page Numbers.
- Federman, A. D., Soones, T., DE Cherrie, L. V., Leff, B., & Siu, A. L. (2018). Association of a Bundled Hospital-at-Home and 30-Day Post-Acute Transitional Care Program with Clinical Outcomes and Patient Experiences. JAMA Intern Med, 178(8), 1033–1040. doi:10.1001/jamainternmed.2018.256
- Title of Paper. (2020). Building the Infrastructure for Rapid Implementation of High-Value Home-Care Delivery Models. JAGS, 68, 1400-1401. © 2020 The American Geriatrics Society. 0002-8614/20.
|
| | |
The Narrow Network Conundrum: Admit or Transfer and the No Surprises Act” | Madisyn Schmitz, JD, MHSA, RHIA, CPC | |
Richelle Marting, JD, MHSA, RHIA, CPC
Member, ACPA Government Affairs Committee
| | |
|
This article is written for educational purposes and is not intended to constitute legal advice. Issues surrounding admission and transfer involving the emergency department can be complex and your legal counsel should be consulted for your own organizational strategy.
A growing trend in the industry is for health insurers to form narrow networks by contracting with a select few providers, which typically include less than one third of eligible providers in a given geographic location. The Government Affairs Committee recently discussed this trend and the implications of transferring patients from a facility outside of the plan’s narrow network to another location in the plan’s narrow network. After all, emergency departments have long been aware of such implications because of the risks of transferring patients due to EMTALA restrictions and concerns for patient dumping from lack of insurance or adequate insurance coverage.
Picture this: a patient presents to the ED with chest pain, and initial workup reveals elevated troponin, and the working diagnosis is AMI. The Emergency Physician contacts the Hospitalist who agrees with the plan to admit the patient. Subsequently, an order is entered for inpatient status and the patient’s health plan is notified of the admission. The response is returned: denied. But, unlike many inpatient status denials tied to the health plan’s interpretation of the two-midnight rule or their own criteria (Review ACPA’s GAC Town Hall for strategies to manage plans’ use of the two-midnight rule), this denial is different. Inpatient status here was denied because your hospital isn’t in-network with the patient’s health plan.
What next? Under the lens of EMTALA, a patient has presented to the emergency department requesting evaluation or treatment. The patient has presumably received a medical screening examination by a qualified professional who determined an emergency medical condition existed. Upon that determination, the hospital has an obligation to: provide stabilizing treatment regardless of the patient’s insurance status or ability to pay. The ability to transfer is only prompted by the initial hospital’s inability to treat the patient’s emergency medical condition. However, if the patient is stable, one hospital may transfer the patient to another facility. If an admission is denied by the health plan for being an out of network facility, the transfer from one hospital to another is being initiated while the patient is registered to the ED, and there is always uncertainty and risk when transferring from the emergency department. Even with the best documentation surrounding the patient’s stability, “stability” is subjective and if the receiving facility finds the patient unstable, the transferring facility risks an EMTALA complaint.
A delay in admission can create implications for accreditation. The Joint Commission integrates performance measurement data into their accreditation process. Performance measures for the ED include the median time from ED arrival to ED departure for admitted ED patients and admit decision time to ED departure time for admitted patients. Delayed decision time on admit or transfer for a patient who has a narrow network could make the performance on these performance measurements worse.
But consider this: you may actually have a health plan in violation of the federal No Surprises Act, Medicare Advantage rules, and/or potentially your state law’s equivalents. Under the No Surprises Act, health plans must generally cover emergency services in a hospital and post-stabilization services. Further, they must do so without requiring prior authorization. The facility should ultimately be paid what is called the qualified payment amount – an amount determined by a formula under No Surprises Act regulations to inform health plans on payment amounts since there is no contracted rate between the plan and the hospital being excluded from a narrow network.
The No Surprises Act applies to group health plans, health insurance issuers offering group or individual health insurance coverage, and carriers in the FEHB Program. Nearly identical requirements to cover and pay for emergency and post-stabilization services apply to Medicare Advantage plans and are also usually addressed under state Medicaid and Medicaid Managed Care organization plans. CMS offers a great FAQ with contact information to ask questions about state or federal laws. The No Surprises Act is managed and enforced by CMS.
-
To submit a complaint of a plan’s potential violation of the No Surprises Act, visit this CMS site. Your organization will help determine whether you should proceed with admission, or determine a stable patient is appropriate for transfer to another facility.
-
A list of state Department of Insurance contact numbers and links to each agency’s website is available here.
-
A list of state Medicaid agencies and links to their websites to locate contact information can be found here.
-
ACPA has shared information on how to use the CMS complaint process to report instances of MA plan non-compliance with rules and requirements here.
Your system’s risk management or legal counsel should be consulted to help evaluate what risk is more reasonable when dealing with narrow networks: risk an EMTALA complaint even if unfounded, or risk not being paid for admitting the patient. Alongside whichever path your organization chooses, there are parallel means of addressing the issue through filing complaints with CMS, the Department of Insurance, state Medicaid agencies, etc.
|
| | |
Dr. Hirsch’s Ramblings on Regulations – April/May 2025 | |
Ronald Hirsch, MD, FACP, ACPA-C, CHRI
Member, ACPA Advisory Board
| | |
|
We are barely 4 months into 2025 and we already have to start looking to 2026 with the release of the 2026 Medicare Advantage Final Rule (CMS-4208-F) and the 2026 Inpatient Prospective Payment Proposed Rule (CMS-1833-P). Neither rule is easy reading, but every physician advisor should find these rules (at www.regulations.gov) and at least read the Executive Summary to see the topics that will be addressed in more depth in the body of the rule. Your roles at your institution can then direct you to determine what warrants closer scrutiny.
For example, I have an aversion to Clinical Documentation Integrity, so I glance over the sections on the proposed changes to DRG assignments and the proposed changes to CCs and MCCs. But clearly any changes to the Two Midnight Rule are critically important so they are carefully sought out throughout the rules as I read. And fortunately, there are no proposed changes.
The bundled payment program TEAM is starting in 2026 and I was quite interested to see what changes CMS is proposing prior to the implementation, and as many have anticipated, CMS is removing the requirements related to reporting health equity measures. CMS did propose to include readmissions of Medicare Advantage patients in their Hospital Readmission Reduction Program. If that is adopted, not only will these readmissions potentially result in a reduced payment for all DRG-based admissions, but you will be doubly penalized by the many MA plans that refuse to pay for readmissions using their own rules. I plan to point this out to CMS in my comments on CMS-1833-P, and I hope many of you will too.
Thanks to the efforts of the past ACPA president Dr. Eddie Hu, who collaborates with people at CMS and the AHA, and members of the ACPA Government Affairs Committee, led by Dr. Ritu Prasad, CMS is also clarifying the regulations around the ability of providers and patients to appeal denials. I will admit I have read that section of CMS-4208-F several times and am still trying to understand it. The CMS rule writers certainly were masters here at making it as incomprehensible as possible. I am hoping that others will read it, understand it, and provide a commonsense interpretation for all ACPA members. I did, though, see that CMS has told MA plans that if they approve an inpatient admission, they cannot go back and deny that admission without good cause. This is clearly a victory for hospitals.
Finally, I want to thank the members of ACPA for awarding me a Distinguished Service Award at the 2025 NPAC. It is easy to do things that you really enjoy, and I really enjoy working with ACPA and educating other physicians and our case management and utilization review colleagues. I am so lucky to have been chosen back in 2006 to be my hospital’s physician advisor; I had no idea that it would lead me to a job and opportunities that I have found so meaningful.
|
| |
|
American College Of Physician Advisors
President's Corner
|
| |
As I reflect on the recent National Physician Advisor Conference (NPAC) that just happened in Chicago April 7-10th- I am struck by how it is always an amazing feeling to be able to spend this amount of time with the physician advisor community. The agenda was a great mix of topics for beginning and experienced physician advisors. And no matter how many sessions I managed to squeeze in, I never felt like I was able to make it to every session I wanted so I am once again grateful for the ability to watch them all through the app after the fact. In fact, I missed the entire first day since I was involved in teaching Essentials and Fundamentals (E&F). Like NPAC itself, E&F has grown so much since the first time we offered it. If you were there, thank you so much for attending! Your attention and questions were great and getting to spend time with early career physician advisors is truly one of my favorite activities.
Of course one of my favorite parts of NPAC is getting to recognize the good work of others. This year Dr. Erica Remer was awarded the Distinguished Service award. She recently stepped down as the Chair of the Clinical Documentation Integrity Committee and the Board at the American College of Physician Advisors. She led the CDI committee’s efforts in their creation of the numerous resources available on the website as well as the townhalls as well as being personally responsible for numerous articles and TLC modules. It is impossible to be involved in CDI as a physician and now know who Dr. Remer is. Thank you, Dr. Remer, for your years of dedication and service!
Dr. Ronald Hirsch was also awarded a Distinguished Service award this year. Dr. Hirsch has served on ACPA’s Advisory Board and his name has been synonymous with the utilization review side of physician advisor work. He received the award this year in appreciation for his long service as Editor for the Newsletter. His work creating the Newsletter and providing his insights in the Editor’s Notes have been invaluable to ACPA members. Thank you, Dr. Hirsch, for your insights and support!
Dr. Dan Zirkman was awarded the Dr. Ronald Rejzer Distinguished Achievement Award. Dr. Zirkman is one of the founding members of ACPA and has been a physician advisor since 2014. He served on the ACPA Board of Directors for 8 years and was also the Learning Center Champion. He continues to support the mission and vision of ACPA and is the Chief Physician Advisor at CarolinaEast Medical Center. Thank you Dr. Zirkman for your time and effort!
In addition to the traditional awards, I added an acknowledgement of our newest members to the Emeritus Board as well as previous inductees. Membership on the Emeritus Board is an honorary title bestowed upon those who have served on the Board with distinction for at least five years and made a significant contribution to the College and is given upon their “retirement” from the Board and leadership from the College. This year’s newest inductees are Dr. Erica Remer and Dr. Alvin Gore (link). Dr. Gore has the distinction of being the longest serving Board of Director member! He has served a variety of roles including Survey Champion and Vice President of Operations. He has provided years of insight and expertise to ACPA and his voice on the Board will be sorely missed.
Additional Emeritus Board members can be found here Emeritus Board.
NPAC itself was great. I got a chance to talk to so many of you! The talks are always the “reason” for the conference, but the people are the “point.” From old friends to new friends, this was the largest NPAC ever! As the industry grows and matures, it strikes me how many more leadership positions there are for physician advisors. The number of colleagues with titles such as lead physician advisor, chief physician advisor, VPs of Physician Advisor Services, etc. seem to only be growing and with it, an increasing need for education on not just how to be a physician advisor, but how to lead a physician advisor team. I think there is still a lot of knowledge to share on that front, maybe a topic for next year’s NPAC? Speaking of which, I can’t wait to see you all at #NPAC2026 in Charlotte, North Carolina!
The CPAL program (The Cultivating Physician Advisor Leaders) wrapped up its pilot cohort recently as well. Thank you to all who participated as mentors or mentees! Mentorship is a core value of ACPA and being able to take something that has always happened and be able to see if finally become a formalized program has been a true privilege for me. We’ll be taking all the feedback and then opening it up for applications this summer for an estimated launch date for the second cohort of late August/early September.
If you’re interested in being more involved in ACPA and leadership, keep an eye out for the VP of Education position which will be posted soon. This is a NEW position and will be a welcome addition to the Executive Committee. Feel free to reach out with questions!
Finally- HAPPY NATIONAL PHYSICIAN ADVISOR DAY!! May 7, 2025, is the second annual celebration. We here at ACPA are proud of you and the work you do! So, THANK YOU and I hope you get a moment to celebrate! As always, please let us know as the professional home for physician advisors what else we can do to support you.
| |
Clarissa Barnes, MD, MBA, FACP, ACPA-C
President, ACPA
|
| |
Thank You to Our NPAC 2025 Top-Level Sponsors! | | |
The American College of Physician Advisors (ACPA) publishes and distributes materials created by our members and speakers for the benefit of all ACPA members. ACPA does not certify the accuracy or authority of these materials. These materials are distributed and presented as research information to be used by ACPA members, in conjunction with other research deemed necessary, in the exercise of ACPA members’ independent professional judgment. Original and fully-current sources of authority should be researched by ACPA members. ACPA disclaims all liability in relation to reliance on the content of these materials. The views expressed in the materials are the views of the material's authors and do not represent the views of ACPA. Any references are provided for informational purposes only and do not constitute endorsement of any sources. |
| | | |