|
|

|
|
I hope this newsletter finds you and your family well. Although the weather still doesn't feel particularly spring-like (second month in a row for that comment), it's still a great time to be a sports fan in Milwaukee. The Bucks are into the second round for the first time in years and the Brewers are on a 10 game home stand. It's a great time to get out to the ballpark and thank goodness for the roof!
Can psychological trauma cause a broken heart? Can stress make us more prone to cardiovascular disease? Is it all in our head? The first article this month explores the relationship between psychological trauma, stress and cardiovascular disease.
We all know that exercise is good and makes us live longer. How does the amount of exercise done during adolescence, early, middle, and later adulthood affect all-cause mortality? Is exercise during one time of life more important than other times? Can it be too late to start? The second article explores this question.
Should we read to our children (or grandchildren) on tablets or e-readers? Is the e-bedtime story in our future? The third study examined parent-toddler pairs reading from both print and electronic books. There is a difference. Check out the third article to learn more.
Click on the links the the left to check out our
web site
.
|
|
Stress Can Break Your Heart
|
Exposure to psychological trauma associated with increased risk of cardiovascular disease

We have had a number of studies showing an increased risk of heart disease in people with depression, but what about other psychological stresses? This large study assessed the association between stress-related disorders including acute stress reaction, post traumatic stress disorder (PTSD), and adjustment disorder and the subsequent diagnosis of cardiovascular disease over 27 years. They compared siblings and matched controls. Findings included a 64% increase between siblings and 71% increase compared to controls in the first year after onset of a major stress disorder. This relationship was especially strong in people under age 50.
Abstract:
- Objective To assess the association between stress related disorders and subsequent risk of cardiovascular disease.
- Design Population based, sibling controlled cohort study.
- Setting Population of Sweden.
- Participants 136,637 patients in the Swedish National Patient Register with stress related disorders, including post-traumatic stress disorder (PTSD), acute stress reaction, adjustment disorder, and other stress reactions, from 1987 to 2013; 171,314 unaffected full siblings of these patients; and 1,366,370 matched unexposed people from the general population.
- Main outcome measures Primary diagnosis of incident cardiovascular disease-any or specific subtypes (ischaemic heart disease, cerebrovascular disease, emboli/thrombosis, hypertensive diseases, heart failure, arrhythmia/conduction disorder, and fatal cardiovascular disease)-and 16 individual diagnoses of cardiovascular disease. Hazard ratios for cardiovascular disease were derived from Cox models, after controlling for multiple confounders.
- Results During up to 27 years of follow-up, the crude incidence rate of any cardiovascular disease was 10.5, 8.4, and 6.9 per 1000 person years among exposed patients, their unaffected full siblings, and the matched unexposed individuals, respectively. In sibling based comparisons, the hazard ratio for any cardiovascular disease was 1.64 (95% confidence interval 1.45 to 1.84), with the highest subtype specific hazard ratio observed for heart failure (6.95, 1.88 to 25.68), during the first year after the diagnosis of any stress related disorder. Beyond one year, the hazard ratios became lower (overall 1.29, 1.24 to 1.34), ranging from 1.12 (1.04 to 1.21) for arrhythmia to 2.02 (1.45 to 2.82) for artery thrombosis/embolus. Stress related disorders were more strongly associated with early onset cardiovascular diseases (hazard ratio 1.40 (1.32 to 1.49) for attained age <50) than later onset ones (1.24 (1.18 to 1.30) for attained age ≥50; P for difference=0.002). Except for fatal cardiovascular diseases, these associations were not modified by the presence of psychiatric comorbidity. Analyses within the population matched cohort yielded similar results (hazard ratio 1.71 (1.59 to 1.83) for any cardiovascular disease during the first year of follow-up and 1.36 (1.33 to 1.39) thereafter).
- Conclusion Stress related disorders are robustly associated with multiple types of cardiovascular disease, independently of familial background, history of somatic/psychiatric diseases, and psychiatric comorbidity.
The term takotsubo cardiomyopathy is known as "broken heart syndrome". It is where an emotional stress causes an ischemic cardiomyopathy. This study looked at different stressors and showed that t
he time immediately after the diagnosis of a psychiatric disorder induced by stress or trauma is a vulnerable time for heart disease risk. This is especially profound in people under age 50 who showed a 49% higher risk of cardiovascular events.
We will all likely be exposed to some sort of psychological stress or trauma in our lives. It is important for us and our physicians to understand that we are at higher risk of physical disease during this time period, especially during the first year after the event. It makes sense that in screening for heart disease we should be asking about nutrition, exercise, smoking, and stress. We should be especially aware of potential increased risk for victims of childhood psychological trauma as they may be at increased risk of premature cardiovascular disease.
|
|
|
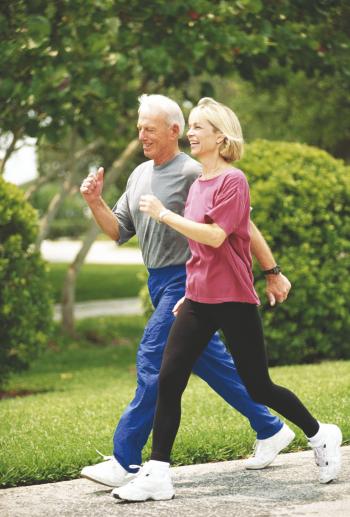
Physical activity reduces mortality, even if started later in life
We all know that exercise is good and reduces mortality. But can it be too late to start? Is exercise during one time of life more important than other times? This article exported these questions by analyzing data from over 315,000 AARP members living in 6 states. Not surprisingly, the authors found that the group who maintained the highest level of leisure time physical activity (LTPA) had the lowest risk of all-cause mortality (36% lower than the least active group). Those who were less active in earlier adulthood but increased activity later in life (ages 40-61) also had similar findings with 35% lower all-cause mortality, 43% decreased cardiovascular death and 16% lower cancer mortality.
Abstract:
- Importance Although the benefits of leisure-time physical activity (LTPA) in middle age are established, the health effects of long-term participation and changes in LTPA between adolescence and middle age have not been documented.
- Objective To determine whether an association exists between LTPA life course patterns and mortality.
- Design, Setting, and Participants This prospective cohort study used data from the National Institutes of Health-AARP (formerly American Association of Retired Persons) Diet and Health Study established in 1995 to 1996. Data analysis was conducted from March 2017 through February 2018. Data were analyzed for 315,059 adult AARP members living in 6 states, namely, California, Florida, Louisiana, New Jersey, North Carolina, or Pennsylvania, or 2 metropolitan areas, Atlanta, Georgia, or Detroit, Michigan.
- Exposures Self-reported LTPA (hours per week) at the baseline interview for ages grouped as 15 to 18, 19 to 29, 35 to 39, and 40 to 61 years.
- Main Outcomes and Measures All-cause, cardiovascular disease (CVD)-related, and cancer-related mortality records available through December 31, 2011.
- Results Of 315,059 participants, 183,451 (58.2%) were men, and the participants were 50 to 71 years of age at enrollment. Ten LTPA trajectories (categorized as maintaining, increasing, and decreasing LTPA across time) were identified, and 71,377 deaths due to all causes, 22,219 deaths due to CVD, and 16,388 deaths due to cancer occurred. Compared with participants who were consistently inactive throughout adulthood, participants who maintained the highest amount of LTPA in each age period were at lower risks for all-cause, CVD-related, and cancer-related mortality. For example, compared with participants who were consistently inactive, maintaining higher amounts of LTPA was associated with lower all-cause (hazard ratio [HR], 0.64; 95% CI, 0.60-0.68), CVD-related (HR, 0.58; 95% CI, 0.53-0.64), and cancer-related (HR, 0.86; 95% CI, 0.77-0.97) mortality. Adults who were less active throughout most of the adult life course but increased LTPA in later adulthood (40-61 years of age) also had lower risk for all-cause (HR, 0.65; 95% CI, 0.62-0.68), CVD-related (HR, 0.57; 95% CI, 0.53-0.61), and cancer-related (HR, 0.84; 95% CI, 0.77-0.92) mortality.
- Conclusions and Relevance Maintaining higher LTPA levels and increasing LTPA in later adulthood were associated with comparable low risk of mortality, suggesting that midlife is not too late to start physical activity. Inactive adults may be encouraged to be more active, whereas young adults who are already active may strive to maintain their activity level as they get older.
Is it ever too late to start exercising? This study shows us the answer is a resounding NO. Exercise is the best way for us to live longer, live healthier, and avoid chronic disease. I have highlighted studies in previous newsletters showing that early adulthood exercise reduces later morbidity. This study shows us that those who are regular exercisers earlier in life but become sedentary do lose a great deal of the protection. On the other hand, this study show us that even people who are not active until age 60 can still have signficant effects on their mortality, reducing the risks close to the levels of people who exercised their entire lives. You are never too old to start!
|
|
The e-Bedtime Story
|
Differences in Parent-Toddler interactions with print vs e-books

Should we read to our children on tablets or e-readers? This study compared parent-toddler pairs reading on three book formats, the enhanced electronic (sound effects and animation), basic electronic, and print. The researchers found less collaboration and verbalization with electronic books as compared to print book reading.
Abstract:
- OBJECTIVES: Previous research has documented less dialogic interaction between parents and preschoolers during electronic-book reading versus print. Parent-toddler interactions around commercially available tablet-based books have not been described. We examined parent-toddler verbal and nonverbal interactions when reading electronic versus print books.
- METHODS: We conducted a videotaped, laboratory-based, counterbalanced study of 37 parent-toddler dyads reading on 3 book formats (enhanced electronic [sound effects and/or animation], basic electronic, and print). We coded verbalizations in 10-second intervals for parents (dialogic, nondialogic, text reading, format related, negative format-related directives, and off task) and children (book related, negative, and off task). Shared positive affect and collaborative book reading were coded on a scale of 1 to 5 (5 = high). Proc Genmod and Proc Mixed analyzed within-subjects variance by book format.
- RESULTS: Parents showed significantly more dialogic (print 11.9; enhanced 6.2 [P < .001]; basic 8.3 [P < .001]), text-reading (print 14.3; enhanced 10.6 [P = .003]; basic 14.4 [P < .001]), off-task (print 2.3; enhanced 1.3 [P = .007]), and total (29.5; enhanced 28.1 [P = .003]; basic 29.3 [P = .005]) verbalizations with print books and fewer format-related verbalizations (print 1.9; enhanced 10.0 [P < .001]; basic 8.3 [P < .001]). Toddlers showed more book-related verbalizations (print 15.0; enhanced 11.5 [P < .001]; basic 12.5 [P = .005]), total verbalizations (print 18.8; enhanced 13.8 [P < .001]; basic 15.3 [P < .001]), and higher collaboration scores (print 3.1; enhanced 2.7 [P = .004]; basic 2.8 [P = .02]) with print-book reading.
- CONCLUSIONS: Parents and toddlers verbalized less with electronic books, and collaboration was lower. Future studies should examine specific aspects of tablet-book design that support parent-child interaction. Pediatricians may wish to continue promoting shared reading of print books, particularly for toddlers and younger children.
Most of us are transitioning away from printed books and magazines to e-readers, tablets and phones for our consumption of written media. How does this transition affect our relationship with young children and grandchildren? I found this study interesting in that parents reading to their young children interacted less with the children when using electronic readers. Some had sound effects which may have reduced parental need for effects and perhaps led to less interaction. But there was also less collaboration and interaction. Overall, it seems that we become more passive in our interactions when they are through electronic media. There is something about the physicality of books - touching and feeling them that seems to cause us to interact with them more and possibly provide better comprehension. Additionally, the blue light from some electronic devices could adversely affect sleep. While there are certainly reasons to use e-readers (travel, etc), perhaps for now we should continue to use old-fashioned books when reading to our children and grandchildren.
|
|
Thank you for taking the time to read through this newsletter. I hope you have found this information useful as we work together to optimize your health. Feel free to pass this on to anyone you think would benefit from this information.
You can find previous newsletters archived on my website here.
As always, if you have questions about anything in this newsletter or have topics you would like me to address, please feel free to contact me by
email
, phone, or just stop by!
To Your Good Health,
Mark Niedfeldt, M.D.
|
|
|