|
I’m back. Happy New Year! Good to see you. Thank you for joining me.
Currently Charmer has +70 committees and groups looking at policy options. I can’t believe it, he’s only gone and done it again… another one.
He must have a process fetish!
Rather than following the very sensible recommendations of the 2011, Dilnot report …
... he's set up another group to look at adult Social Care. Led by cross-bencher, Baroness Louise Casey.
She did Boris’ homelessness report and worked on rough-sleeping. Alas, not much changed. This time, she’s doesn’t have to hand in her homework until 2028... bonkers.
Let’s speed things up. Write Ms Casey's report, right now;
‘With an ageing population the costs for caring for the elderly are out of control. It has to be fixed because it is the cause of all the delay, misery and expense for families - silting-up the wider performance of the NHS.
The public know this.
They are cross at the thought of houses being sold in exchange for often, indifferent care. Add dementia to the mix and relatives are soon at their whit’s end to know what to do.
The state must step in, and quickly, to do six things;
1 Turn social care jobs into careers with training, qualifications, pay scales and promotion.
2 Define a care-staff minimum wage, above the general minimum to encourage recruitment (already under way).
3 Make the sector viable for care companies with evidence-based, ring-fenced £ allocations for adult social care.
4 Cap the amount that individuals are expected to pay for care-home occupancy. For example, say; £80k (?). A cap creates an insurable risk for people and families and avoids the need to sell a house.
5 Where possible and there are willing volunteers, train and pay members of the family to become carers, much as they do in Germany (Pflegegeld service), and in Sweden, the Netherlands, Austria, Germany, France, Italy and some US States.
6 The interface between health and social care has to be frictionless. Setting up a new organisation (National Care Service) will make it worse. Another silo. Better to incorporate adult social care into a beefed-up NHS community and primary-care to provide a one-stop service, with integrated data.’
Simples. Right, now we've got our sleeves rolled up and we’re in the mood, what else?
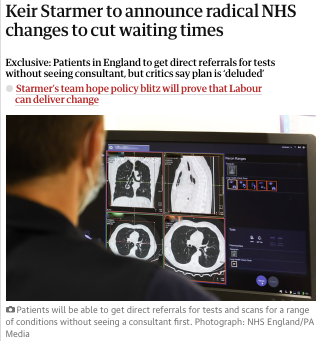
By all accounts Charmer is to announce 'fast-track referrals' for some diagnostics and, for hospitals who make the fastest improvements in reducing waiting times (not lists) a share of 'millions for buildings and equipment'.
Here's the point.
About 60% of people waiting need one or more diagnostics. Of them only 20% will need a period of inpatient care.
That means the rest might need outpatient or day-case follow-up, or importantly... nothing.
Kicking the ‘nothings’ off the list will reduce the numbers waiting... but all the rest will still be in a queue for something or other.
The reward schtick is an old Milburn wheeze and just makes things worse.
Good hospitals get better and the strugglers don’t. Being a struggler is largely a matter of legacy, geography and finance. Investing in 'the strugglers' is the way to make progress and level-up the service.
Rewards also create, perverse incentives. The temptation to cherry-pick ‘easy’ patients...
... which leads to gaming the system…
... which leads to the neglect of quality, patient satisfaction and a host of other unmeasured metrics.
Plus, national performance targets cannot take account of local variations in demand, overlooks capacity constraints, demographics, population health and staffing issues. Making incentives unrealistic or counterproductive for some hospitals.
Turning rewards and running a hospital into a game show with 'prizes', ignores investment strategies. And ignores the real system-flow issues. Not to mention morale.
Another re-tread in Charmer's package is Milburn's Choose and Book fiasco, of 2005; 'a choice of hospitals', mired in technical chaos
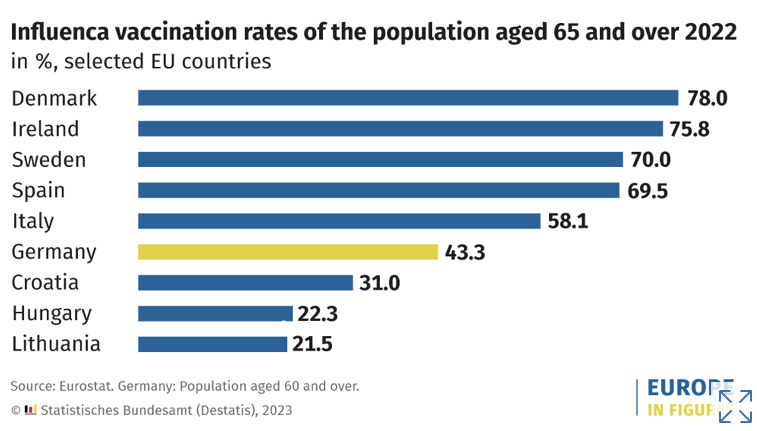
We know from the last time we tried this, aside from hugely complex software requirements, travel is a principle concern for 9 out of ten patients. The biggest group of waiters is predominantly the over 65ys. Especially the +75ys, where chose and travel is a non-starter(Fig 8).
People prefer ‘close to home' for ease of access, reduced travel time, and lower associated costs. That’s why NHSE has another other policy, ‘care closer to home’.
It's really not a goer and...
... it doesn't fix the unspoken problem. Which is;
...about +300k join NHS waiting lists every month and about +300k leave. You either increase productivity with innovation, workforce and investment in poorer performing care locations or stop people getting sick in the first place.
That means...
... invest in primary and preventative care for principly the +65's and the -5yrs, to avoid admissions and help slicker discharge.
That means...
... guess what... invest in social care, which takes us full circle…
… and where we came in, this morning.
Is this a ‘new year’ or have we been here before?
|