|
To the sound of an electronic bompety bomp, wha-wha, and a cloud of white smoke, the blue police box manifested at Pier Head waterfront, Liverpool.
… out steps Andy Burnham…
… he’s wearing a tie… he’s Blighty’s new prime minister.
His time machine has moved us to Sunday, 27th September, just in time for the Labour Party Conference.
What’s he gonna do?
Loadsa-stuff? Probably not. The markets are spooked about more borrowing. We’re still suffering the collateral damage of Trump's wars and his attempts at redefining geopolitics and the meaning of the word ‘peace’.
At the conference, Andy will cheer us up… that might be enough for now.
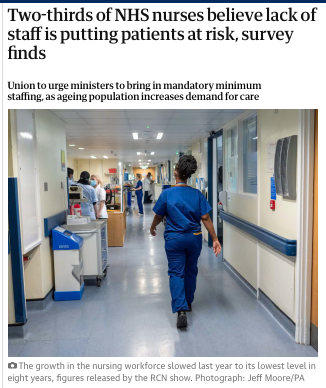
Oh, and the NHS?
Politicians always promise to ‘save the NHS’… while quietly presiding over a system that has become less and less national and more risky with variation.
The clue is in the name; National Health Service.
The NHS is not really a single organisation. It's a federation of semi-independent institutions; trusts, foundation trusts, regulators, commissioners, arm’s-length bodies and oversight agencies…
... all linked together by contracts, targets, meetings and increasingly desperate coordination.
From the outside, it looks national.
From the inside, it behaves more like a loose holding company.
If I were to place a bet, I’d say this might be the first thing he’d try to change. Maximum impact at relatively little cost.
Not by nationalising the NHS in the old-fashioned sense, but by putting the national back into it.
The Thatcher reforms, later reinforced by Blair’s markets and turbocharged by Lansley, created hospitals and trusts that are effectively sovereign organisations.
Each with its own board, executives, procurement systems, strategies, auditors, lawyers, communications teams and priorities.
In theory autonomy was meant to create innovation and responsiveness.
Instead, the NHS has drifted into something awkward; pseudo-markets with huge overheads. Time and money spent managing the interfaces between organisations that are all ultimately funded by the taxpayer.
That may have been manageable when we had loadsa-money and demand was stable. Not now.
Burnham might start by simplifying the architecture.
Trust boards and their surrounding governance machinery probably costs somewhere around £5m a year for a large acute trust.
There are about 250 Trusts = £1,250,000,000 and sorry to say; looking at quality indicators, productivity and finance, many are ineffective, governors ignored. Only half are rated good.
Presently, the NHS is drifting towards the chaotic merger of NHSE and the DH+, done properly it could be the basis of a Burnham reorganisation…
… his instincts are civic rather than managerial. He’s always understood something Westminster often forgets…
… institutions need a story people can recognise and feel part of. Now, the NHS has no narrative.
Which brings us to one of the more interesting possibilities.
If you reduce the power and number of NHS boards, how do local communities retain influence?
Let’s bring back the Community Health Councils.
The decision to dismantle Healthwatch England may accidentally create the space for precisely that debate.
Healthwatch never really captured public imagination or authority. The old CHCs, for all their faults, at least felt rooted in communities and independent of the machinery they scrutinised… mad-Milburn dumped them.
A Burnham version might be different… beefed-up civic watchdogs, building relationships, informed by live operational data, and …
… that leads to the future of the CQC.
The uncomfortable truth is the CQC has never convincingly improved quality. It inspects after failure has become visible. Now, no one with any sense will work there. It’s falling apart.
NHS decline is usually predictable long before inspectors arrive…
- staff turnover,
- sickness rates,
- agency spending,
- corridor care,
- complaints,
- leadership churn,
- poor flow,
- whistleblowing,
- maternity warning signs…
… the signals are almost always there.
A Burnham NHS might junk this and replace it with continuous-system-sensing; local, civic scrutiny backed by predictive data and earlier intervention.
Not inspection as theatre. Quality surveillance as intelligence. It’s a profound philosophical shift.
The last thirty years treated the NHS as a regulated market. Burnham might treat it as a public service, centrally coordinated, locally accountable, digitally integrated and publicly visible.
The danger is, centralisation can suffocate initiative just as fragmentation creates chaos.
It’s the Goldilocks paradox…
too much local freedom and the system fractures;
too much national control and it freezes.
Burnham might try to discover where the balance really belongs.
|