|
It’s an outrage!
Hold the front page…
… that's what the £walled Sunday Times did when they discovered a hospital advertising for ‘corridor-care nurses’… the ad’ was previously on Twitter. (More here).
The rest of the media piled-in.
Presumably only skinny nurses need apply so they can squeeze past the catering trolleys, porters with patients in wheelchairs, a juggernaut of laundry…
… and procession of relatives looking for their granny.
As unacceptable as corridor care is, it has been a ‘thing’ since Covid. The NHS call it ‘temporary escalation spaces’… which of course makes everything sound... ‘managed’ and ok.
There’s indignation that valiant NHS estates people are plumbing in electricity and oxygen connectors, in corridors.
‘Normalising’ poor care.
No. It's pragmatic and sensible, to prevent the dangers of trailing extension cables and the risk of oxygen cylinders. They've also been fitting curtains.
People got out of their prams when they discovered, corridor-nurses will be employed on 12 hour shifts… too long, too arduous and dangerously-exhausting they cried.
Please realise, 12hr shifts have been common since the 1980s and 90s, here, in the US and a lot of European systems.
It reduces handover costs and longer shifts can improve continuity of care. Staff shortages made 12hrs shifts part of a solution and nurses with families and second jobs seem to want it. Some don't and say it's unsafe.
Whatever, it’s a thing. Get over it.
Notable for his absence, over the weekend is our great leader…
… the RCN and others have have reminded us…
… on taking up his role as secretary of state for health Wes Streeting promised to ‘end corridor care in the NHS’.
Good luck with that, Wes... probably why he's in hiding.
Time to recognise reality, the cost of your inaction on social care and how different campaigning is when compared with actually doing the job.
Time to start thanking hospitals for their innovation, initiative and quick responses.
As ugly as we all think it is, turning corridors, cupboards and in some cases offices, into safer, if undignified places, where the tsunami of patients can be looked after with some sort of structure by people who know what they’re doing, is pragmatic at the very least...
... and at most, in a perverse sort of way, the NHS at its best.
Streeting, has been invisible since the furore started. He knows he can only drivel on about a ten year plan and something on social care by 2028.
There is nothing he can do. Well, maybe he could make sure the 30/40 new hospital programmes build places with wider corridors?
Sensibly, right now, there's nothing anyone can do, more than is being done…
... other than saying thank you and well done for trying to keep us as safe as possible in incredibly difficult circumstances.
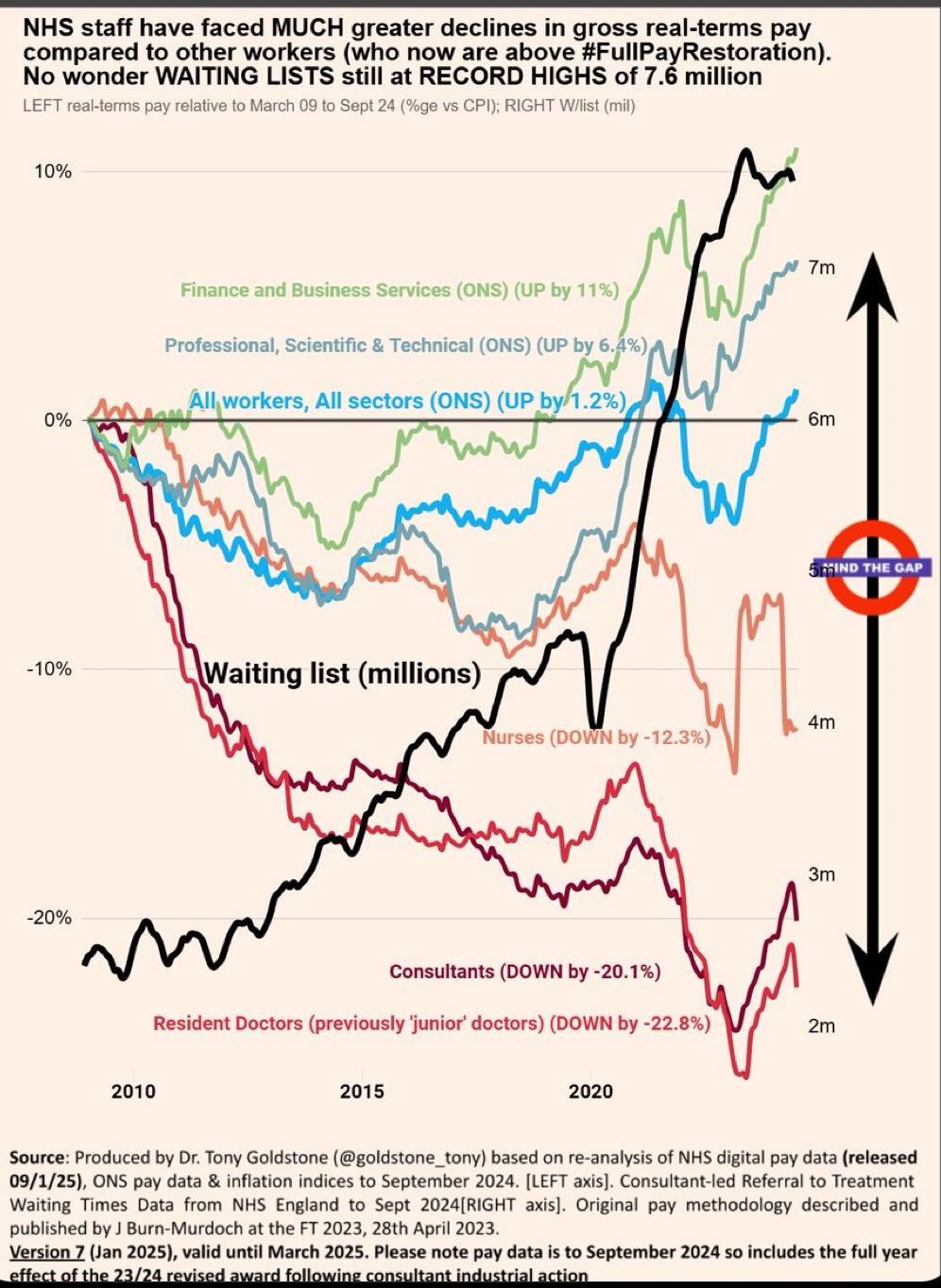
The NHS runs at close to capacity most of the time, around +90%. Safe levels are down in the eighties. Capacity is the euphemism for choc-a-bloc and the upshot is yer granny in a cupboard.
An immediate injection of cash into emergency community teams might help, but is likely too little, too late. As would be a push on vaccinations, masks and ventilation.
Commandeering beds from Wes’s friends in the private sector might help but they only have 8,000, mostly in wealthy areas. If they have to cancel operations to admit NHS medical patients, they’ll be looking at contractual issues and compensation… it’d probably need legislation.
Bring in the Army?
The army is already ‘in’. The days of military hospitals are long-gone. Military nurses and doctors already work side-by-side with the NHS.
When real leaders are faced with difficult and intractable situations what do they do?
-
Reframe the problem; this is not a hospital problem it is a community and social care problem, so stop bad-mouthing hospitals.
-
Break it down; start with frailty indices and figure out how to make them meaningful.
-
Challenge assumptions; that this has to happen every year.
-
Find collaborators; stop picking fights and blame-shaming.
-
Involve diverse groups; employers could they help with family emergency leave, experts, families with experience, community leaders, gather insights, thoughts, ask for help.
-
Encourage cross-sector partnerships; schools, clubs, fire services, postal workers, retired NHS people, football clubs.
-
Find small, local initiatives; see if they are scale-able, replicable.
-
Recognise this is a dynamic problem; solutions will have to be iterated.
-
Not every experiment will succeed; so learn.
-
Reinforce core community systems; to withstand uncertainty.
-
Leverage Technology and Innovation; to keep people safe at home.
-
Look globally; for solutions.
-
Acknowledge complexity; be honest about the problem and the difficulties.
Share and celebrate success.
Try and inspire confidence, highlight commitment and success. Build a shared vision of what solutions looks like. Empower people and inspire hope.
Stop hiding Wes, be a leader, not a blamer.
|