|
|
|
|
|
Brain Injuries
|
| In recent years, sports-related brain injuries have become a major area of scientific investigation. Clinical research developments in neuroimaging have heightened public awareness, spurring greater industry action and regulation on the issue of better protecting players. The National Football League (NFL), for example, has been on the hot seat lately with lawsuits from former players alleging that it intentionally and fraudulently misrepresented and concealed medical evidence about the risks associated with traumatic brain injuries (TBI). The consequences of these injuries range from short-term effects, like dizziness and nausea, to long-term effects, like depression, dementia, and memory loss. Research has also indicated that repetitive concussive and subconcussive blows to the head in sports like football, hockey, and soccer increase athletes' risk of developing neurodegenerative diseases like chronic traumatic encephalopathy (CTE). While these new findings on CTE have captured the public limelight, other less visible areas of brain injury research are also making great headway both in the U.S. and in Germany.
Brain injuries can be classified into three main categories. Traumatic brain injuries, for example, are alterations in brain function caused by external forces, such as a fall, motor vehicle crash, gunshot wound, or a violent blow to the head or body. Acquired brain injuries (ABI), on the other hand, are neurological injuries that are neither hereditary, congenital, nor degenerative in nature; they are also not induced by birth trauma. Rather, this type of brain injury occurs after birth, such as by cerebral vascular accidents (commonly known as stroke) or by loss of oxygen to the brain (referred to as hypoxic brain injury). For brain injuries that are not considered to be traumatic or acquired, a third grouping exists for injuries either present at birth, such as cerebral palsy, or progressive in nature, like Alzheimer's and Parkinson's disease.
Both mild and severe brain injuries pose a variety of serious implications, including impaired functioning in neurologic, endocrine, neuromuscular, orthopedic, and/or neuropsychiatric areas. Researchers in Germany are tackling these issues head-on with a spectrum of holistic solutions ranging from preventive care, such as with stylish, flexible helmets designed to encourage usage, to recovery efforts, as with serious games intended to increase patient adherence to rehabilitation training.
|
|
|
|
|
 |
|
|
Source: � Brainlab AG
This past year, one of Europe's largest university hospitals, the Charit� - Universit�tsmedizin Berlin, was the first clinic in Europe to use a mobile computed tomography (CT) scanner. Airo�, the cohesive imaging and patient positioning solution, is ideal for cranial, spine, and trauma procedures, making it a highly versatile intraoperative imaging system. Its high CT image quality increases surgeon confidence and supports advanced minimally invasive surgery.
Designed to function inside existing operating room (OR) suites, Airo boasts an ultra-small footprint. Innovative design intelligently combines the largest gantry opening on the market with a slim gantry that houses custom components like an X-Ray tube, 32-slice helical scan detector array, high-voltage generator, air-cooling system, and built-in battery pack.
The Airo electrical drive system is suspension-controlled and features a solo central wheel for compact maneuvering. Equipped with user-friendly control software, even one person can easily move Airo from OR to OR. The front-view safety camera also helps ensure stress-free mobility.
The compact Airo system pendant controls everything. During procedures, surgeons and staff program imaging with laser alignment and dose display from the detachable and user-friendly touch screen. Movement and maintenance are also swift and steady with the Airo handheld system controller commanding transport, daily calibration, and system maintenance.
Airo is distributed by Brainlab, a German medical technology company based in Munich. Brainlab develops, manufactures, and markets software-driven medical technology, enabling access to advanced, less invasive patient treatments. Brainlab technology powers treatments in radiosurgery as well as neurosurgery and other surgical fields.
To find out what is trending in neuronavigation, radiotherapy, and the healthcare industry in general, follow Brainlab on social media via Twitter, Facebook, LinkedIn, and YouTube.
Airo is manufactured by Mobius Imaging, LLC. On June 17, 2014, Mobius Imaging was awarded gold in the Radiological and Electromechanical Device category of the 17th Annual Medical Design Excellence Awards (MDEA) competition for Airo Mobile Intraoperative CT.
Image owned by Brainlab AG
|
|
|
|
A study by the Association of the German Insurance Association revealed that 90 percent of all head injuries in bicycle accidents occurred on the bottom rim of the skull. Unfortunately, this is exactly where many helmets fail to provide sufficient protection, according to Florian Mayer, an industrial design student at the Pforzheim University of Applied Sciences in Germany. Florian Mayer has created an innovative, aesthetically pleasing new helmet design called TheRove "14/57." Its slightly modified structure protects the sides and the back of the head better than pre-existing helmet models. The individual helmet sections are held firmly together with flexible leather Kevlar belts. Furthermore, the helmet's super shock absorbing material, composed of visco-elastic foam padding, can be bended, folded, and even rolled. "The [head] protection can roll up to a small size," Mayer said, outlining one of the most important features of his model - that it is both portable and easy to stow. Product "14/57" is part of the brand concept TheRove, developed by a collaboration of artists, designers, and clients. Its product portfolio consists of bicycles, accessories, and everyday objects of urban life and culture. TheRove envisions the helmet as a new category of accessory for cyclists of the future.
To view Florian Mayer's design portfolio online, click here. To watch a video interview (in German) with the designer about the helmet, click here.
Source & Image: � FMD |
|
|
|
One in six people worldwide will have a stroke during their lifetime. Many survivors experience their most dramatic recovery during their hospital stay in the weeks following their stroke. But other survivors also continue to improve over a longer period of time, sometimes over a number of years.
The goal of rehabilitation after a stroke is to help survivors regain as much independence and quality of life as possible. Rehabilitation cannot reverse brain damage. However, high quality rehabilitation is essential for regaining many - if not all - capabilities needed to lead a meaningful, fulfilling, and even productive life.
The best results are achieved in specialized rehabilitation centers with consistent support from doctors and therapists. Effective rehabilitation must be intensive and repetitive. However, the increasing costs of the healthcare system are leading to time limits in clinics, which are not always sufficient for creating lasting changes. Additionally, after returning home, patients often lack the motivation and discipline to continue systematic training.
The Rehab@Home project, based on collaborative research funded by the European Union Seventh Framework Programme, aims at enabling healthy aging through engaging rehabilitation. Rehab@Home offers a cost-effective, sleek infrastructure with integrated sensors that collect relevant physical and medical information on a patient's status for checkups and relapse prevention. Smart sensors in the device's cameras and control units track the patient's movements during a video game, enabling doctors and therapists to provide feedback online. Doctors can access the data to monitor the patient's progress in order to adapt his or her training plan and give further necessary instructions.
As in every video game, patients work their way up from level to level, receiving instant gratification, encouragement, and motivation when achieving their exercise training goals. Patients are also encouraged to share their achievements with family and friends and can even challenge each other in online training contests on the Rehab@Home platform.
To learn more, visit: www.rehabathome-project.eu or email Prof. Dr. Michael Lawo ([email protected]) at the University of Bremen.
Source & Image: � Rehab@Home
|
|
|
|
Prof. Dr. Ulf Ziemann is a leading German expert on clinical neurophysiology, stroke, multiple sclerosis, movement disorders, and peripheral neurology. He currently serves as Chairman of the Department of Neurology and Stroke at the University Hospital T�bingen and as Director of the Hertie Institute for Clinical Brain Research at the University of T�bingen. In 2014, he was featured on a list of the best physicians in Germany.
In his interview with GCRI, Prof. Dr. Ziemann describes the main types of strokes as well as which of these are most common. He also elaborates on the short- and long-term effects of a stroke and the impact his research on noninvasive brain stimulation (NIBS) techniques has had as a novel model for neurorehabilitation. Finally, he discusses which research projects he would like to focus on next. To read the full interview, click here.
Prior to his roles at the University of T�bingen, Prof. Dr. Ziemann served as Associate Professor and Vice Chairman of the Department of Neurology at the Goethe University Frankfurt am Main from 2004 to 2012. Former international career highlights include time abroad as a volunteer at the National Institute of Neurological Disorders and Stroke (NINDS) and the National Institutes of Health (NIH) in Bethesda, Maryland as well as a Visiting Fellow at the Institute of Neurology in London, U.K. In 1991, Prof. Dr. Ziemann received his medical degree from the University of G�ttingen, Germany.
Prof. Dr. Ziemann is author of 252 peer-reviewed publications, 38 book chapters, and six books. His research expertise concerns the human motor cortex, excitability, plasticity, motor learning, transcranial magnetic stimulation (TMS), non-invasive brain stimulation, brain-state dependent stimulation, closed-loop stimulation, neuropharmacology, TMS-EEG, and neuroimaging.
Recognized for his excellence in neurology, Prof. Dr. Ziemann has received numerous accolades, including the 2006 Richard Jung Award of the German Society of Clinical Neurophysiology, the 1999 NIH Merit Award, and the 1998 NIH Fellowship for Research Excellence.
Image: � Hertie Institute for Clinical Brain Research |
|
|
|
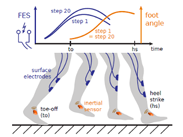
Many people have walking deficits after suffering a stroke. Foot drop, i.e. insufficient dorsiflexion of the foot during the swing phase of gait, is a frequent phenomenon, which is conventionally treated by passive ankle-foot orthoses. Functional electrical stimulation (FES) represents an advantageous alternative for supporting weak motor functions. However, most commercially available stimulators are not individually tailored for the user. Typically, a simple heel switch inside the shoe triggers the stimulation, which is then applied with constant intensity during the swing phase. For such systems, the stimulation intensity either needs frequent manual adjustment or must be set to an unnecessarily high value, which causes abnormal foot motions and rapid fatigue of the stimulated muscles. These problems can be overcome if the foot motion is measured and used to adjust the stimulation intensity automatically as the patient walks. Due to the repetitive nature of gait, it is particularly promising to employ iterative learning control (ILC) techniques for these adjustments. The success of such control schemes critically depends on the real-time assessment of foot motion. Researchers at the Technische Universit�t Berlin in cooperation with partners at the Charit� - Universit�tsmedizin Berlin and HASOMED GmbH have investigated two different sensor technologies for performing these measurements. One approach uses bioimpedance measurements via skin electrodes. An alternative approach equips the shoe or foot with an inertial sensor, which enables foot orientation measurements. By attaching a second inertial sensor to the shank, it is also possible to calculate the dorsiflexion ankle joint angle. With ILC, a time varying stimulation intensity profile is applied during each step. This profile is adjusted at the end of each swing phase. These updates are based on the difference between the desired and the recorded foot angle profile during the previous step. To learn more, click here. To watch a video of one of the experiments, click here.
This research project is funded by the TU Berlin, the German Federal Ministry of Education and Research (BMBF), and the Max Planck Society.
Source & Image: � Thomas Seel, Technische Universit�t Berlin |
|
|
|
|
|
|

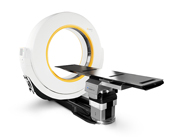
 Airo-Mobile Intraoperative CT Scanner
Airo-Mobile Intraoperative CT Scanner