Weekly News From Los Alamos County
August 4, 2022
|
|
Inside this newsletter, you will find...
The Epidemiology Corner - COVID-19 Update, COVID Plateau, Hope for the Future
of the Pandemic, Aug 8 Vaccine Clinic, Survey & Results, COVID-19 data, and more.
|
|
|
|
COVID-19 Update: Community Transmision and Emergency Department Visits Remain Comparatively High
in the County...
|
|
Highly Transmissible and Immune-Evasive BA.5 Variant Causing Most U.S. Cases, But BA.4.6 Variant Emerging
For the week ending July 30, CDC estimates Omicron variants BA.4/BA.5 accounted for 93% of U.S. cases nationwide, with BA.5 alone accounting for 86% of cases. CDC is also tracking a new variant of concern termed BA.4.6, which has been gradually increasing in the U.S., and now accounts for about 4% of cases nationwide. See HERE. The ability of the BA.4.6 variant to outcompete BA.5 and other circulating variants is unclear, as is it’s ability to evade immunity conferred by current vaccines or prior infection. See HERE. New hospital admissions for COVID-19 declined slightly in the U.S. during the week ending July 30, suggesting that a peak may be forming, but additional data going into August are needed to confirm. Health authorities remain concerned that the fall return-to-school and more indoor crowding may result in increased community transmission and a possible need for more restrictive prevention measures. However, most U.S. public schools are poised to begin the upcoming school year with a mask optional plan. See HERE.
|
|
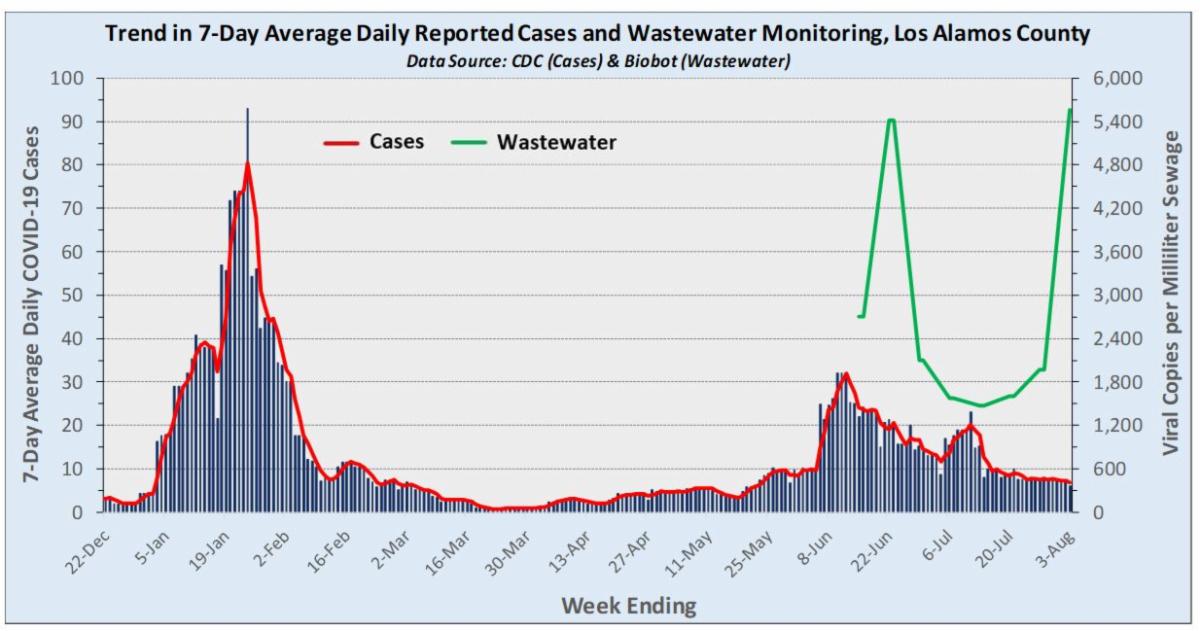
COVID-19 in the County: Reported Daily Cases Continue Gradual Decline But Community Transmission Still Comparatively High
Average daily reported cases continue to decline from the recent early June peak, but community transmission remains comparatively high. An average of 6.1 cases per day were reported for the week ending August 3, which represents a roughly 20% decline from the 7.7 daily cases reported the prior week. In comparison, an average of one case per day was being reported in the county during late-March/early-April 2022. For samples collected the week ending July 20, the CDC-contractor conducting wastewater surveillance in the county (Biobot), reports the BA.5 variant accounted for essentially all viral copies (100%) detected in sewage. See https://biobot.io/data/ Inexplicably, the most recent measured level of virus in wastewater markedly reversed the declining trend which appeared to be accompanying the declining trend in average daily case counts. Interpretation of such a major reversal is difficult given the lack of long-term monitoring data for comparison purposes.
|
|
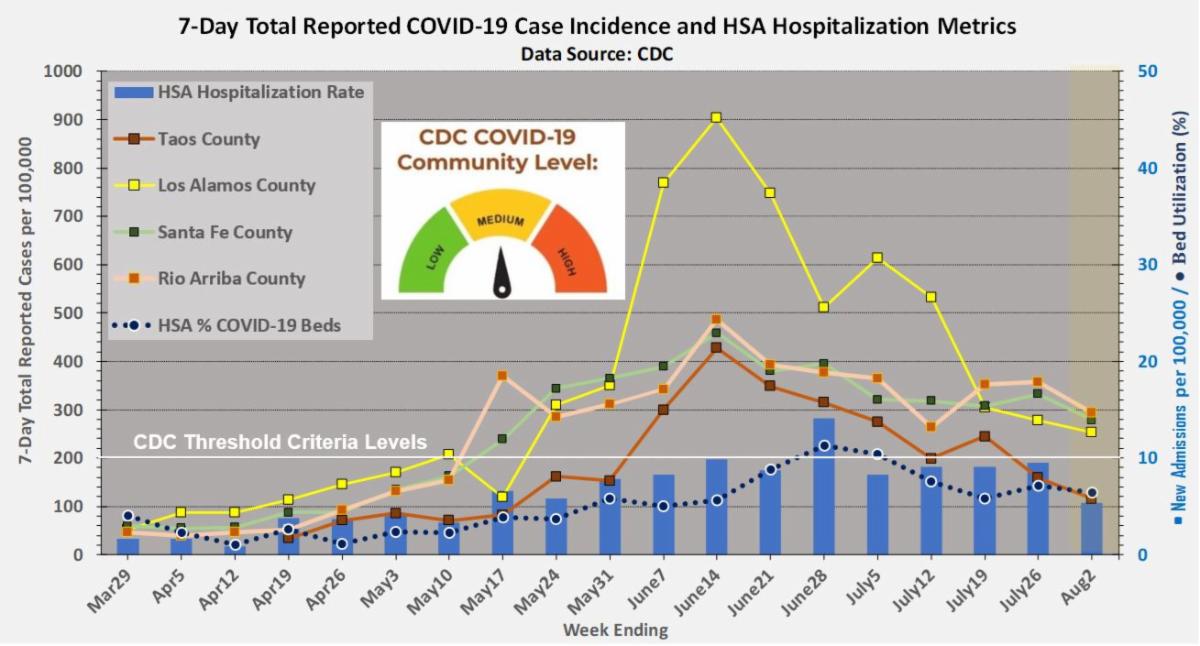
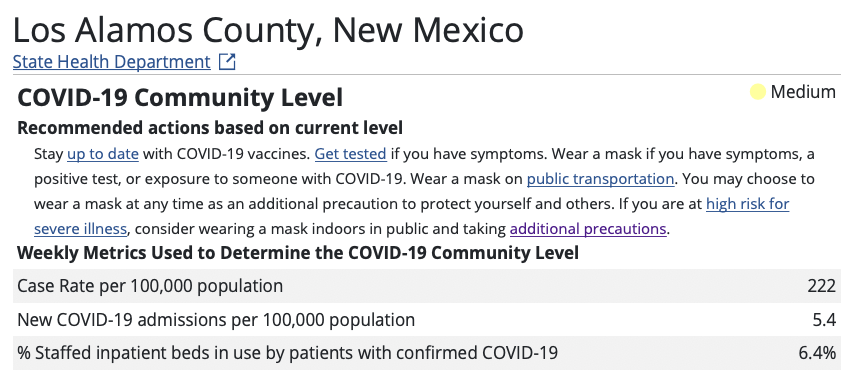
CDC Community Level Risk MEDIUM But Transmission Risk Remains Comparatively High
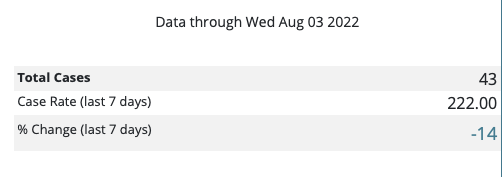
For the week ending August 2, the CDC Community Level remains at MEDIUM. Health Services Area (HSA) hospitalization metrics have notably improved as case incidence rates in all four HSA counties continue to decline. Compared to the prior week, the rate of new COVID-19 hospital admissions declined by roughly half from 9.5 to 5.4 new admissions per 100,000. The reported case incidence in Los Alamos County (222 per 100,000 as of August 3) remains slightly above the CDC criteria threshold of 200 cases per 100,000, and is at a level comparable to that seen in the three neighboring HSA counties (Santa Fe, Taos, Rio Arriba). Although gradually declining, community transmission rates in the county still remain well above those seen in late-March 2022.
|
|
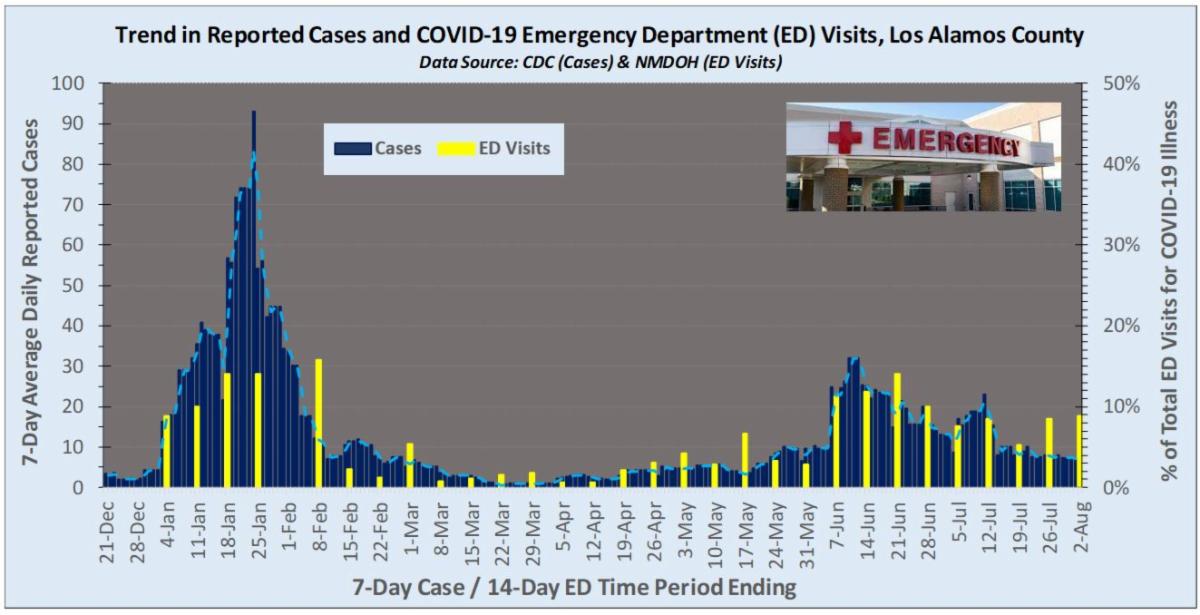
Emergency Department (ED) Visits for COVID-19 Symptoms Remain Comparatively High in the County
As reported by NMDOH, the percentage of all ED visits for COVID-like illness in County residents has varied over time with the number of reported cases, and currently remains elevated around 8% compared to the 1%-2% range seen in March-April 2022. COVID-like illness includes ED encounters with chief complaint consisting of fever and cough, shortness of breath, or difficulty breathing, while also including COVID-19 associated discharge diagnoses codes. The definition excludes known influenza related ED visits coded with a related influenza discharge diagnosis. See HERE. ED visits for COVID-like illness in the County would be expected to decline with continued declines in average daily reported cases. At the same time, the large recent increase in wastewater SARS-CoV-2 viral levels noted above leaves open the possibility that sustained high ED visit measures, along with high wastewater monitoring levels, might signal a reversal in trend towards higher community transmission.
|
|
NOTE: The COVID-19 incidence data reviewed here are based on PCR-confirmed testing results compiled by CDC and NMDOH and do not include data on positive at-home antigen tests. As such, case counts are likely underestimated, but how much cannot be determined at any given time point.
To assist with more complete case monitoring in New Mexico, NMDOH provides for online reporting of positive at-home antigen results HERE.
|
|
|
Do you have children starting school soon?
|
|
No, but I have immediate family that does.
|
|
|
|
|
|
|
US stuck in a 'horrible plateau' of COVID-19 deaths, experts say. Here's why.
"COVID is over" might trend within social media circles, but weekly U.S. death tolls tell a different story.
The pace of COVID-19 deaths has remained relatively steady since May, despite an uptick in July to about 400 a day, according to a USA TODAY analysis of Johns Hopkins University data.
“We’re sitting on this horrible plateau,” said Dr. Daniel Griffin, an infectious disease specialist with Pro Health Care in New York and a clinical instructor of medicine at Columbia University. “It’s been this way for the past couple of months, and we’re getting used to it.”
In July, more than 12,500 Americans died of COVID-19, according to the USA TODAY analysis.
Coronavirus deaths are similar to the number of influenza deaths normally reported during peak season, said David Dowdy, epidemiologist at the Johns Hopkins Bloomberg School of Public Health. A bad flu season in the USA could see more than 50,000 deaths.
That doesn’t mean COVID-19 mortality has reached that of flu, he said, as peak flu season lasts only about three months. Spread over the course of the year, Dowdy said, there would be about four times as many COVID-19 deaths than flu deaths.
COVID-19 is “like having to live in flu season year round, and that’s not what we do with the flu,” he said. “If we had to do that with the flu, we’d be instituting more measures than what we do.”
Most Americans who died of COVID-19 were immunocompromised or older than 75, experts said. These patients ranged in vaccination status – from being unvaccinated to receiving all their recommended vaccines and boosters.
What appears to make the biggest difference between patients who recover from COVID-19 or die, Griffin said, is whether they receive treatment within the first week of diagnosis.
“I can’t remember someone in my recent memory who did all the right things, who got the vaccine and got the proper early treatment, and ended up in the hospital and died,” he said.
The antiviral Paxlovid, from Pfizer, has been effective at keeping high-risk COVID-19 patients out of the hospital. But it’s losing esteem among providers and patients as public figures report rebound infections after taking the antiviral, Griffin said.
It’s not clear whether a rebound after taking the antiviral is different from a rebound without the drug. In the trial that led to Paxlovid’s authorization, 2% of those who took the medication and nearly the same percentage of those who didn’t experienced rebounds.
The uncertainty surrounding antivirals and other COVID-19 treatments may contribute to preventable deaths, Griffin said.
“This plateau now, as horrible as it is, is unfortunately lower than it’s going to be if we don’t do a great job this fall with boosters and improving education about how to properly manage COVID,” Griffin said.
To read the full article, click HERE.
|
|
The Three COVID Developments I’m Still Holding Out Hope For
We don’t have to be in this COVID rut forever.
We are in a covid rut. Early on in the pandemic, we could look forward to the arrival of vaccines. But the vaccines came, and though they did wonders in bringing down the daily death toll, COVID is ever present in our lives.
When we step back and assess the news in totality, we might feel that we are stuck, that things aren’t going to get better, and that, no matter what progress we make, the virus will outsmart us sooner or later.
With a virus that has evolved to morph and recirculate with the frequency of the common cold and far greater deadliness, many people are wondering if we’re going to have to live like this forever.
So what could still happen to fundamentally change the COVID big picture? I’ve been thinking about that question, and I’ve come up with three possible good developments that could come down the pike. Here’s what I’m holding out hope for:
1. The virus’s rate of change could slow down.
A virus of exactly the same rate of spread, immune-evasion properties, and severity as COVID-19 would be a lot more tolerable if it mutated at the rate of the flu and surged at more predictable times. Masking for one period a year (for those who still wish to avoid the virus) instead of constantly living in fear would be quite an improvement—and more people might be willing to do it.
Planning and predictability would be nice for everyone, but especially so for people at high risk. Those who are immunocompromised or otherwise high-risk would be released from continual anxiety and could participate more freely in the activities that bring them joy.
So far, there aren’t signs of a slowdown in coronavirus mutations, and the alphanumeric soup of BA variants is coming at us fast. But COVID-19 tends to change in surprising ways that we can’t explain until later. Let’s hope this becomes one of them.
2. An accumulation of layered immunity might render COVID a more tepid illness.
The virus may not ever mutate at a slower pace, but those mutations could become a lot less important. This could happen as layers of immunity—from a combination of prior vaccinations and prior infection—give the virus less and less power to make us really sick. Over time, SARS-CoV-2’s effect on us may come to resemble something closer to the common cold, caused by another, more familiar, coronavirus. COVID-19 wouldn’t disappear, but it would be characterized by mild symptoms that for many would barely register.
This is the path many mistakenly believe is inevitable, one we have already started on. Yet we are not there. We still hold our breath each time a new variant of concern is spotted. In the U.S. alone, some estimates suggest that more than 90 percent of the population has been infected or vaccinated—and still hundreds are dying each day. For us to be at a better place, everyone—including older, frailer, and sicker people—will need to be able to live like the pandemic is over.
3. Science could win.
Although we would all welcome a more predictable disease and more tolerable symptoms, the scenario we really hope for is one in which we don’t need to worry about getting infected at all. For that to happen, we need innovation in vaccines, to make better ones than we have today. A lot of innovations are being developed (including ones that handle a wider range of variants); the most helpful vaccine would prevent us from catching and spreading the virus in the first place.
Such a vaccine is at least a few years away, but more than a dozen candidates are currently in various stages of clinical research (the Russian Ministry of Health claims to have one). These trials are difficult, as there is no accepted measure of immunity other than antibody titers in the blood, which aren’t as relevant here.
We, of course, have had plenty of good news during the life of the pandemic, much of it from the world of science—vaccines have made COVID far less lethal, therapies keep us out of the hospital, and treatments allow more people to leave the hospital if they’re admitted. But good news in the pandemic has had strange properties: Oftentimes it seems not to be exactly as advertised. The virus mounts its own reaction, mutating in ways that can increase severity, as with the Delta variant, or increase transmissibility, as with Omicron. As a result, we have seen enough good-news false starts to know that news can’t be officially declared “good” until months later.
But even if we have plenty of reason to distrust any seemingly good news, we also have plenty of reason to expect the situation to improve. History bears this out. COVID-19 isn’t the first and is hardly the worst virus to prey upon humans. To be sure, many earlier pandemic-causing viruses circulated long beyond their acute initial phase, but the pandemic stages eventually ended, and the damage ebbed as scientists developed better treatments and vaccines and the human body adjusted.
When will this happen with COVID-19? We’ll know six months after it already has.
To read the full article, click HERE.
|
|
Germany announces new Covid measures for fall, expecting another wave of infections
The German government on Wednesday presented its plans for new coronavirus measures for the coming fall and winter as it expects virus cases to go up again during the colder season.
Wearing masks on planes and during long-distance travel by train and bus will be mandatory from October to early April all over Germany. Mandatory mask-wearing and the presentation of a negative coronavirus test will apply to hospitals, nursing homes and similar institutions with vulnerable people.
Many other rules will be implemented individually by the country’s 16 states depending on how severely the virus spreads in their regions. This could include the wearing of masks on local public transportation, in schools for students in grade five and up, and at public indoor events.
Some community facilities such as schools, prisons or asylum-seeker shelters may also implement regular testing again if virus numbers rise, the German health and justice ministers said in a joint statement.
“Germany should be better prepared for the next coronavirus winter than in previous years,” Health Minister Karl Lauterbach said, adding that a vaccination campaign would start in the fall as well, with new vaccines.
Justice Minister Marco Buschmann added that special efforts will be made to keep schools open.
“Children have a right to school education and a school day that is as carefree as possible. School closures must therefore not be allowed,” Buschmann said, adding that states will “only be able to impose a mask requirement at schools if this is necessary in order to be able to continue to provide in-person teaching.”
The new regulations still need to go to Cabinet and parliament but are expected to pass.
|
|
CDC COVID Data Tracker - August 4, 2022
To get today's break down of positive case data, demographics information, vaccine status and more for Los Alamos County or other counties across the United States, click HERE
|
|
The charts available with this TOOL layout the key metrics for understanding the reach and severity of COVID-19 in a given area.
|
|
Johns Hopkins
COVID-19 Status Report Dashboard for
|
|
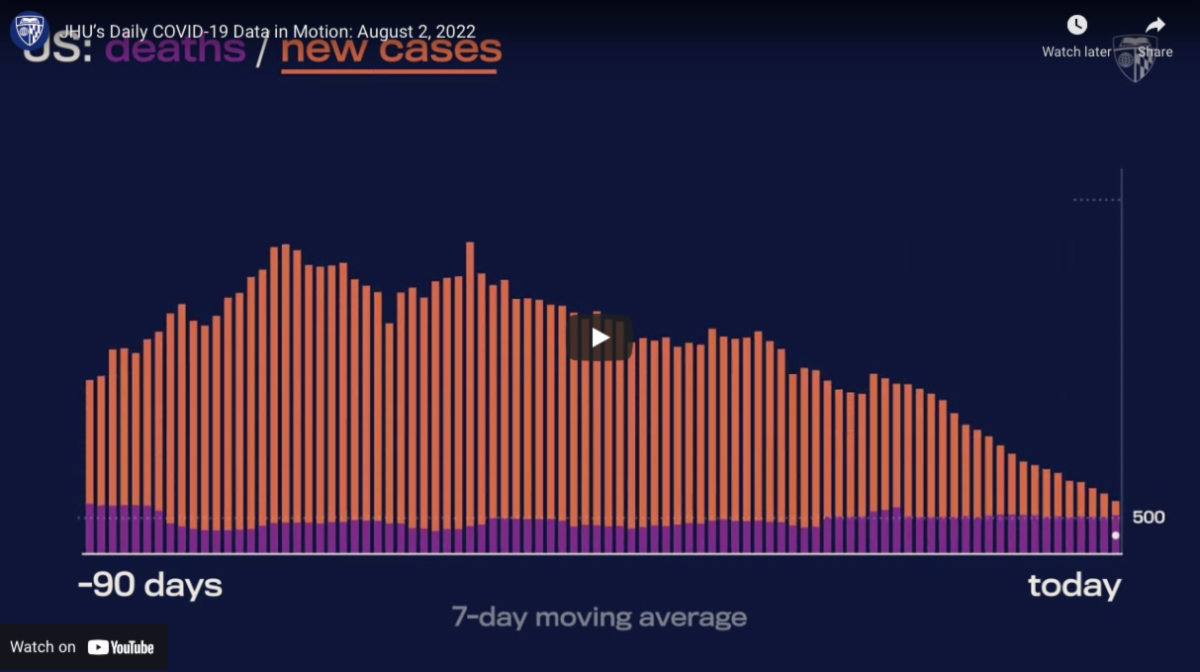
Daily COVID-19 Data in Motion
The Johns Hopkins' Daily COVID-19 Data in Motion report is a 60-second, daily summary of the most important data on COVID-19 in the U.S., updated every morning. The report shares critical data on COVID-19 from the last 24 hours.
|
|
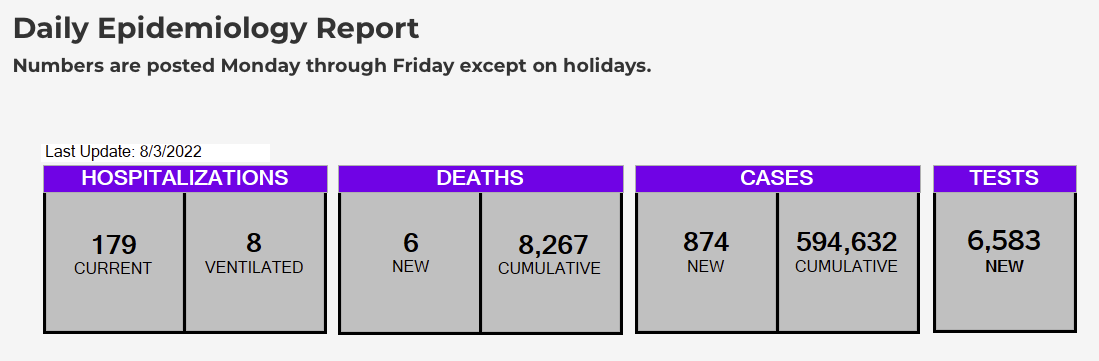
NMDOH Epidemiology Reports - Daily and Weekly Data
As part of the COVID-19 pandemic response, NMDOH collects and analyzes statewide data for COVID-19 positive cases, hospitalizations, and deaths. The reports reflect these critical data and are updated weekly - click HERE
|
|
Los Alamos Vaccine & Booster Information |
|
August 8th COVID-19 vaccine/booster clinic expanded to include all eligible individuals
In conjunction with Los Alamos County, Premier Medical Group (PMG) has expanded the COVID-19 vaccine/booster clinic scheduled for Monday, August 8, to include all eligible individuals, not just children 6 months to 5 years. Between 10 a.m. and 2 p.m., PMG will administer Moderna and Pfizer vaccines at the First Baptist Church, 2200 Diamond Dr., Los Alamos.
Insurance and identification are not required. While walk-ins are accepted, appointments are preferred. Visit the New Mexico Department of Health (NMDOH) vaccine webpage to schedule an appointment. After logging into the appropriate NMDOH profile, individuals are advised to select "schedule an appointment," enter "Los Alamos," and select "First Baptist Church" on the map. No event code is needed.
For those encountering problems scheduling an appointment, NMDOH is available any day of the week from 8 a.m. to 8 p.m. at 1-855-600-3453 to assist. In addition, the Los Alamos Public Health Office is available at 505-662-4038 to help individuals schedule appointments.
|
|
How do I know if I'm eligible for a vaccine or booster?
Follow these links to review the CDC eligibility guidelines:
|
|
Los Alamos County COVID Vaccine/Booster Resources
Visit the County COVID Page for information regarding vaccinations/boosters, click below:
|
|
QUESTION
I got my 2nd Booster at a County sponsored Vaccine Clinic at the end of June, but when I check my VaxView data it only shows 3 shots -- the most recent shot isn't listed. Do you send the data to the state or is there something I'm supposed to do?
|
|
ANSWER
The Vaxview site is run by the New Mexico Department of Health. We are told you should reach out to them via email at COVID.vaccines@state.nm.us to have this corrected.
|
|
We are listening to you!
Your feedback is helping to shape future newsletters, inform decisions regarding services, and make Los Alamos County healthier and safer. Make sure to participate each week to be heard!
|
|
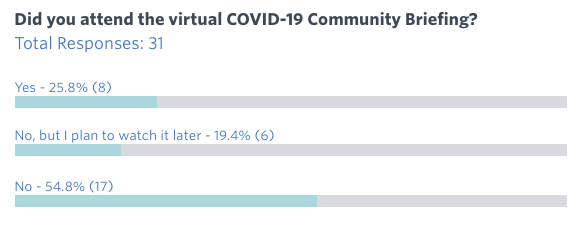
Remember, we appreciate your questions! We always try to respond in a timely manner, and if appropriate, we will include those Q&As in future newsletters.
Take a look at these results from the last survey:
|
|
Have a question? Email us. |
|
Los Alamos Treatment Information |
|
Los Alamos County COVID Treatment Resources
Visit the County COVID Page for information regarding treatments, click below:
|
|
Los Alamos Testing Information |
|
Los Alamos County COVID Testing Resources
Visit the County COVID Page for information regarding testing, click below:
|
|
What else would you like to see in this newsletter?
Click below to email us your feedback and questions!
|
|
|
|
|
|
|