News From Los Alamos County
March 31, 2023
|
|
Inside this newsletter, you will find...
The Epidemiology Corner - COVID-19 Update, It's Time for Your Booster, Three Years In..., All About Long COVID, Weekly Survey, COVID-19 data, and more.
|
|
|
|
COVID-19 Update:
Pandemic Trends Continue to Improve - New XBB.1.9.1 Variant Emerges - FDA Undecided on Spring Booster...
|
|
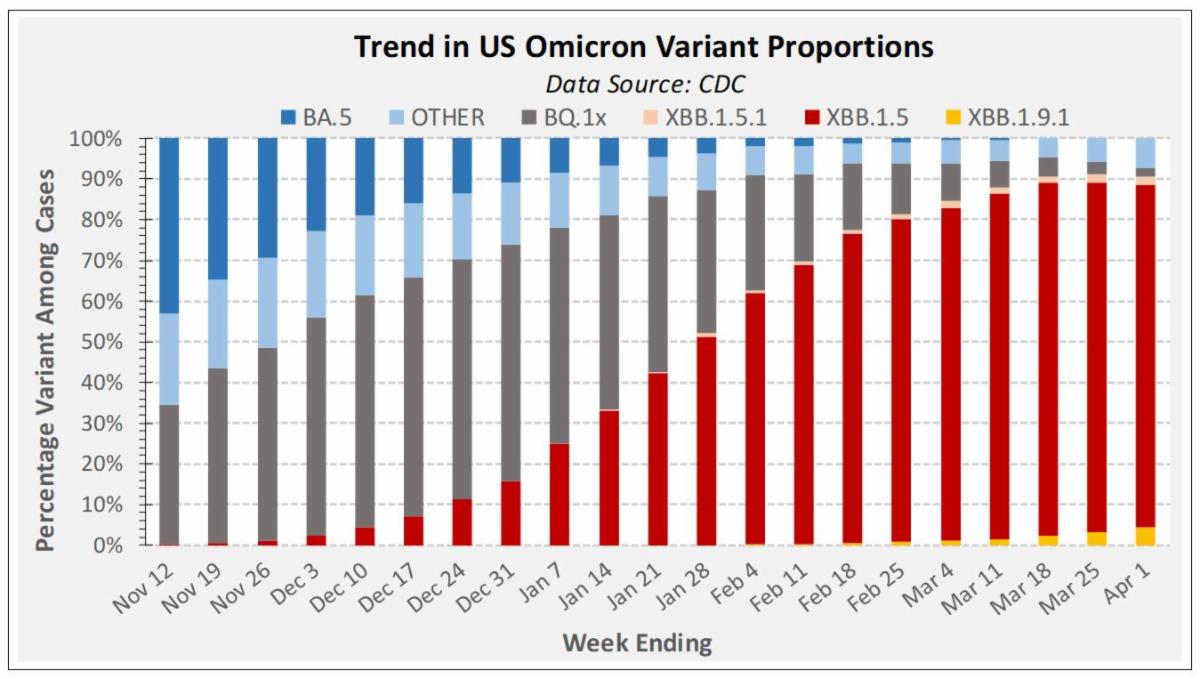
COVID-19 Update: Omicron XBB.1.9.1 Emerges with Apparent Growth Advantage over Prior Variants
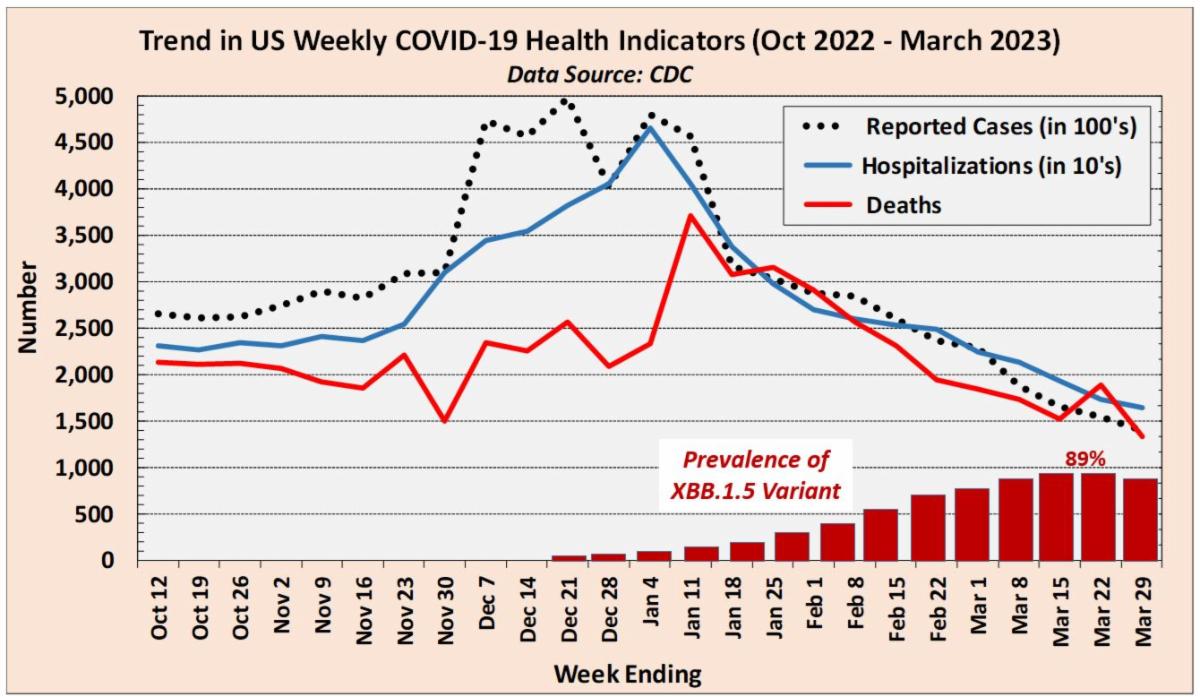
Predominance of the Omicron XBB.1.5 variant is now beginning to slowly wane from a peak 89% prevalence. CDC has begun tracking the ascendant XBB.1.9.1 variant, which appears to have some growth advantage over prior variants. National prevalence of XBB.1.9.1 is now estimated at 4.6%, however strong regional variation exists. Highest prevalence is in the Central Mid-West Region (Iowa, Kansas, Missouri, and Nebraska), where it now accounts for roughly 16% of cases. See Variant Proportions Whereas the XBB.1.5 variant wave was not associated with a surge in hospitalizations and deaths, it’s too early to assess the virulence of the XBB.1.9.1 variant and assume the same benevolence. Early data from other countries where XBB.1.9.1. has emerged more fully, particularly Singapore, do suggest an increased severity. See Variant in Singapore What is clear is that virus is still circulating and infecting people, with the elderly and the immunocompromised being the ones most likely to end up with severe disease. For the week ending March 29, an average of 2,300 Americans were hospitalized per day for COVID-19 and roughly 230 died each day from the disease. The US Food and Drug Administration (FDA) remains undecided on whether a spring bivalent booster shot will be offered in the US. See Spring Booster Other countries, including Canada and the United Kingdom, are offering spring boosters to select high-risk populations, including seniors, elderly residents in congregate assisted care, and persons with compromised immune systems. See Spring Booster Eligibility
|
|
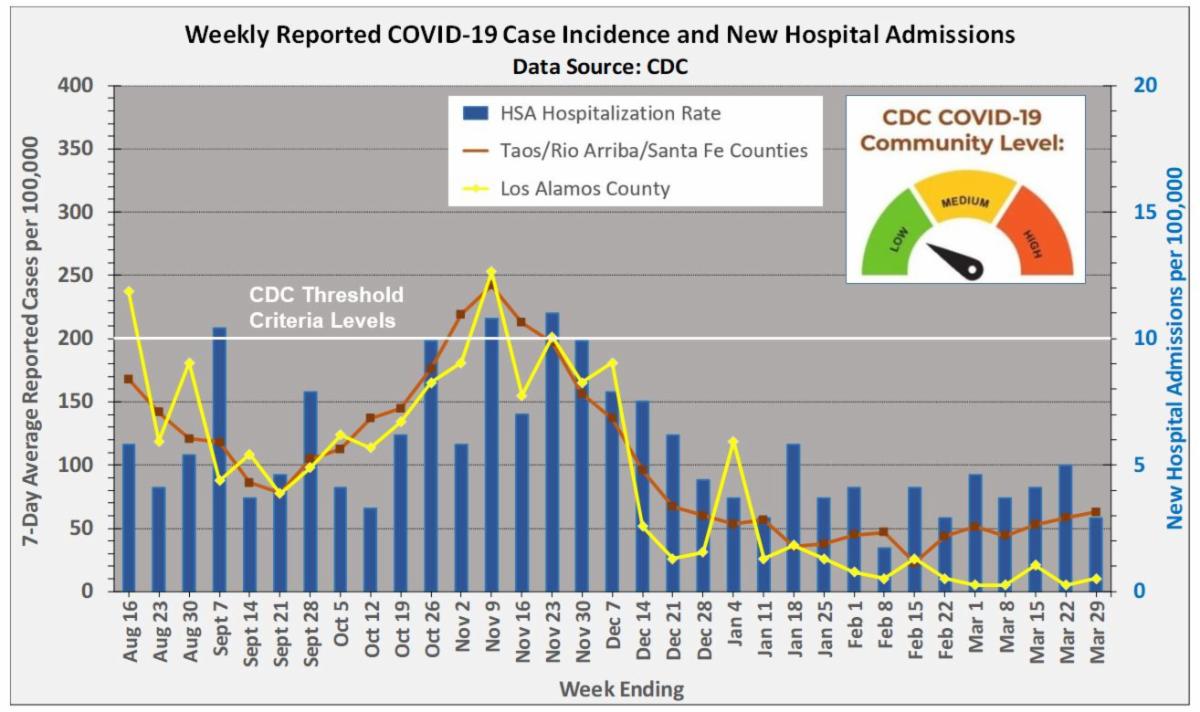
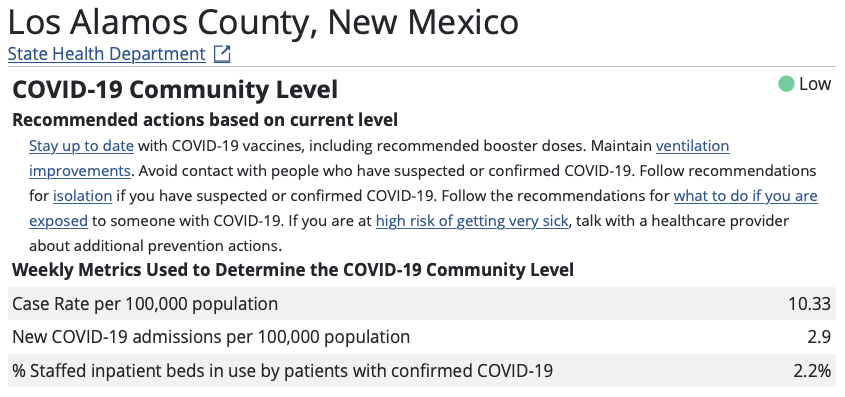
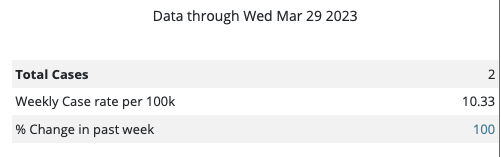
CDC Community Level Risk Remains at LOW for the County as Reported Cases Remain Low
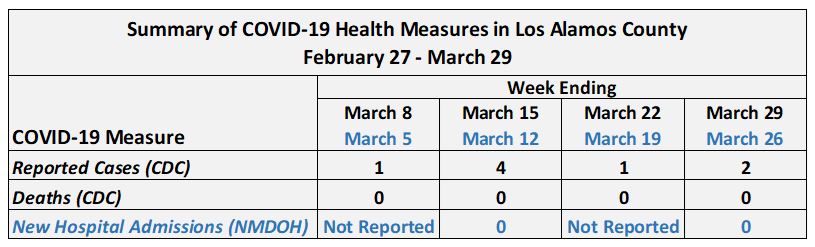
For the week ending March 29, the CDC Community Level remained at LOW for Los Alamos County, as it did for the three other counties (Taos, Rio Arriba, Santa Fe) which collectively comprise the regional Health Services Area (HSA) over which CDC hospitalization metrics are calculated. Reported cases in the county averaged 2 per week for the month of March. Per capita reported incidence for the county remained stably low and varied from 5 to 10 cases per 100,000. In contrast, March saw a continued rise in per capita incidence for the remaining three counties in the HSA. For the week ending March 29, per capita incidence was six-fold higher in the neighboring three-county area (63 per 100,000) compared to Los Alamos County (10 per 100,000). Part of the difference in reported incidence is likely due to the relatively low PCR testing rates in the county. For the roughly three-week period ending March 23, daily per capita PCR testing in Los Alamos averaged 2.6 tests per 10,000 compared to 7.6 tests per 100,000 for Taos, Rio Arriba and Santa Fe counties combined. HSA hospitalization rates remained relatively stable during March, which indicates ongoing transmission and progression to severe disease for some persons. No new hospital admissions among county residents were reported by NMDOH for the month of March.
|
|
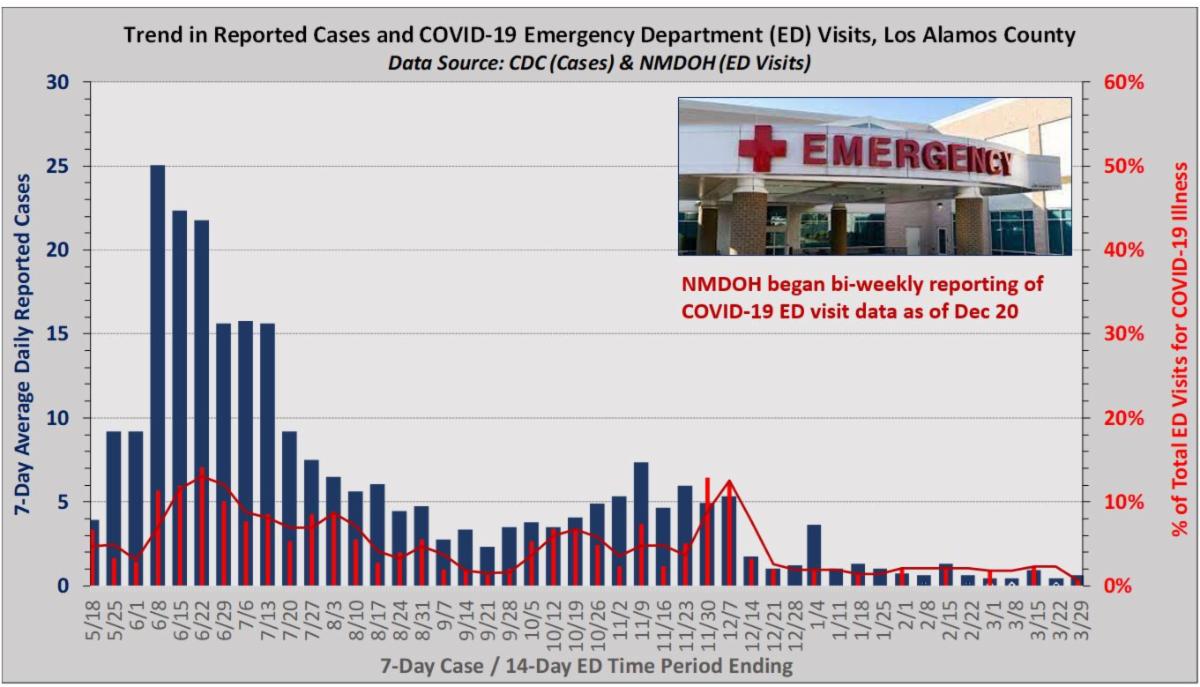
Emergency Department Visits for COVID-Like Illness Remain at Stable Low Level
NMDOH reports the percentage of emergency department (ED) visits in county residents for COVID-like illness declined to 0.7% for the two-week period ending March 28. These data remain indicative of continual low level virus transmission in the community. Statewide, the percentage of ED visits for both COVID-like and flu-like illness remained stable at about 3%. Beginning April 11, 2023, NMDOH will report COVID-19 ED and hospitalization data solely on a monthly basis. See State Report
|
|
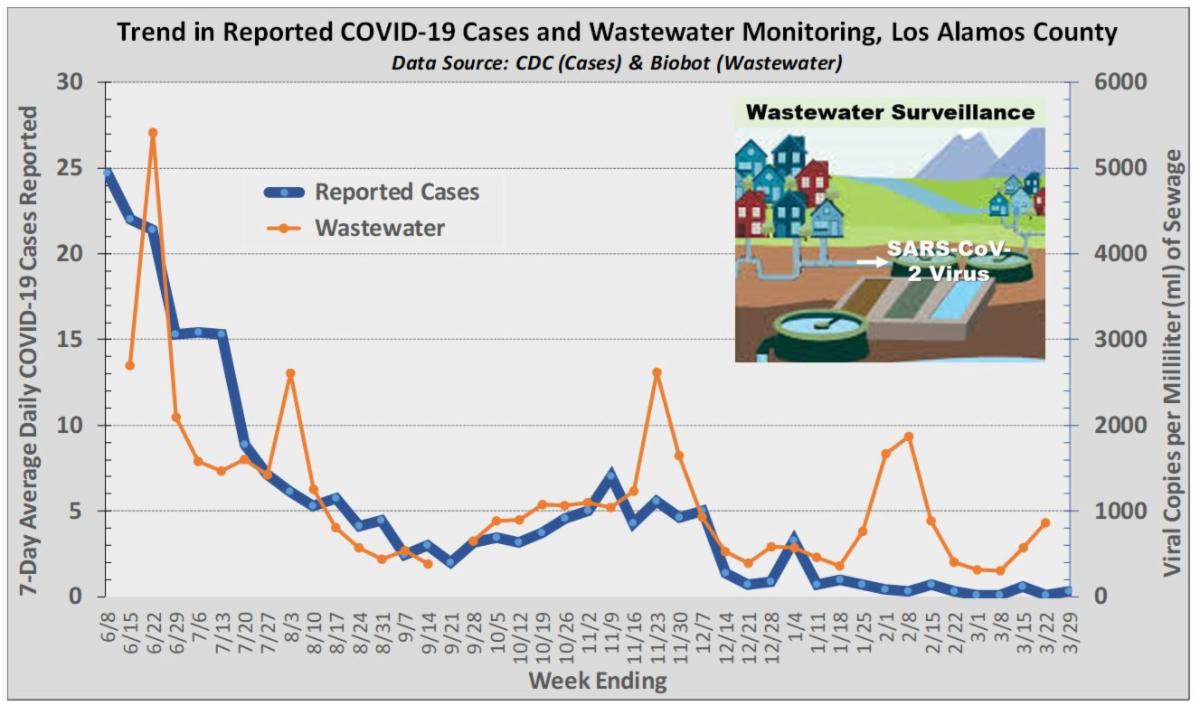
COVID-19 Virus Continues to be Detected in County Wastewater
Data reported by the Biobot contractor through the week of March 22 indicate SARS-CoV-2 virus continues to be detected in county wastewater at levels consistent with on-going community transmission. Amounts of virus detected in county wastewater (copies per milliliter sewage) have generally been similar to that seen nationwide. As of the week of March 13, Omicron XBB variants continue to account for the majority of detected virus in county wastewater. See https://biobot.io/data/
|
|
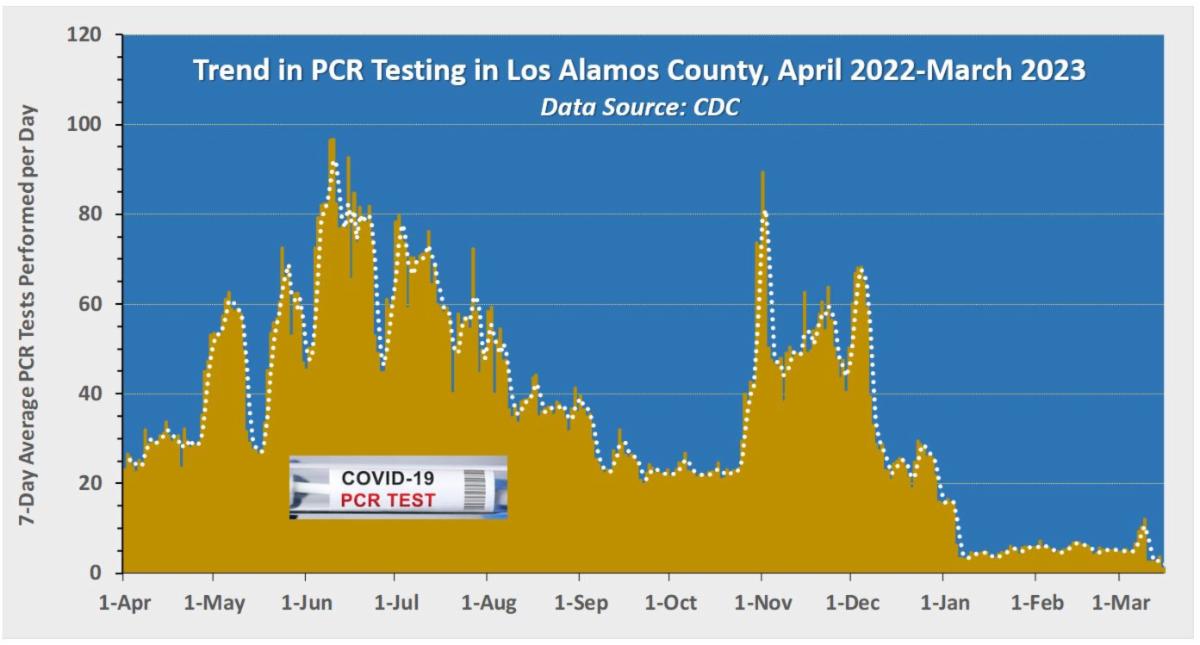
Daily PCR Testing in County Returns to Trend Established in Early 2023
Daily PCR testing in the county returned to trend following a brief upward excursion around the end of the first week of March. This appears to have been due to a one-day spike in testing. For the two-week time period ending March 23, PCR testing averaged about 5 tests per day among county residents.
|
|
New Mexicans Encouraged to Self-Report Positive COVID-19 Home Tests
To assist with more complete case monitoring in New Mexico, NMDOH encourages residents to download the NM Notify app and to report positive COVID-19 home tests on the app, or for a fast and easy way to report your at-home test results online, visit https://makemytestcount.org/.
The NMDOH/CDC COVID-19 incidence data reviewed here are based on PCR-confirmed testing results and do not include data on positive at-home antigen tests. As such, case counts are incomplete and underestimated, but by how much cannot be determined precisely at any given time point.
|
|
Los Alamos Vaccine & Booster Information |
|
Did you know the virus that causes COVID-19 changes over time?
Safeguard your family and friends this autumn by receiving the Omicron booster. The Omicron booster is designed to offer broad protection from the original virus strain and the Omicron variant for everyone 6 months or older. If you’ve received at least two doses* of COVID-19 vaccine and it’s been at least two months, schedule your booster appointment below.
*or one if you received Johnson & Johnson
|
|
Are you eligible for the Omicron booster?
If you meet the criteria above, don’t wait. Schedule your Omicron booster today!
|
|
Los Alamos County COVID Vaccine/Booster Resources
Visit the County COVID Page for more information regarding vaccinations/boosters:
|
|
The state of COVID in the U.S. three years into pandemic
Three years into the pandemic, cases, hospitalizations and deaths are all declining. But questions remain about new variants and whether some people may need a spring booster shot, and there are many concerns about the impact of long COVID.
Epidemiologist Katelyn Jetelina joined William Brangham with an update on the state of COVID in the U.S.
William Brangham:
Geoff, it's worth noting good news when it occurs. And, on COVID, there is some. The U.S. avoided the worst of a winter surge, and weekly recorded deaths from this virus are the lowest they have been since the early weeks of the pandemic.
But it is not all good news. More than 1,700 Americans still died last week because of COVID. And, for the elderly, immunocompromised and those still struggling with the little-understood long COVID, this pandemic is hardly in the rearview mirror.
For another check-in on COVID, we're joined again by epidemiologist Katelyn Jetelina. She's at the University of Texas. And she writes the very informative Substack called Your Local Epidemiologist.
Katelyn, great to have you back on the "NewsHour."
What is your take on where we are in the trajectory of this pandemic? Deaths are down, as I mentioned, but there is this XBB variant that is — subvariant, that is now dominant in this country. Where are we?
Katelyn Jetelina, University of Texas Health Science Center:
You know, it's a really good question.
I think we're somewhere in between a full-blown emergency, like we saw in the beginning of 2020, and somewhere before an endemic. We're just not at a state where we know what this virus is going to do. And this virus is not being very predictable.
Like you said, all metrics are nosediving right now. And that's good news. We expect that to happen with spring because of warmer weather, less holiday gatherings. But COVID continues to do its COVID thing and continues to mutate. It's what viruses do to survive. And we're paying specific attention to XBB offshoots, one in India and one in the U.K. That is causing a little disruption and some smaller waves.
And so this does have the potential to disrupt a quiet spring in the U.S., but it's still too early to know for sure, given our complex immunity landscape.
William Brangham:
Speaking of that immunity landscape, it's been about six to seven months since the bivalent boosters became available, which is plenty of time for a lot of people to have lost some of their protection.
You wrote about this today. Is there good evidence for a spring booster?
Katelyn Jetelina:
I think it depends on what you define as good evidence.
It's really difficult for us to know how much each booster helps or does not help and incrementally, and get a grip on it prospectively. And so what we know for sure is that protection is robust for younger and healthier people, keeping them out of the hospital, which is great news.
The concern is for immunocompromised and older adults with comorbidities. And this is because their immune systems are just not as strong. And it's being — they're being pulled in multiple directions. And so this is a group where we really want to avoid infection in order to prevent hospitalization and death.
And we know these antibodies, like you say, that prevent infection wane pretty quickly and only last about six months.
William Brangham:
And elderly Americans, 65 and older, those are increasingly the people who are still dying of COVID. Isn't that right?
Katelyn Jetelina:
That is correct.
I think the last statistics was about 90 percent of deaths are among those over 65 years old; 96 percent of hospitalizations are among old adults, older adults, with at least one comorbidity, and because, again, their immune systems are just taxed.
I think the good news is that very few people are in the hospital today who are up to date on vaccines. So, the vaccines are working. The essential question is, is this going to change in time? And what do we do proactively?
William Brangham:
I want to touch on long COVID, this still mysterious ailment that so many people are suffering from.
What are we learning about who is getting it and why?
Katelyn Jetelina:
You're right. There's millions of Americans right now debilitated, out of work, suffering, with very few treatment options.
We are starting to get a better grip on what causes COVID. It seems to be several factors, like, for example, a lingering virus or people harbor the virus in their tissue, which can create damage. I know that other people get long COVID driven by the immune system. Autoantibodies just start attacking the body itself.
And then there's also just immune dysregulation, that, even if someone clears the virus, the immune system is off-balance, and so other dormant viruses reactivate and drive chronic symptoms. So, long COVID, we're learning, is really an umbrella term for several causes.
And this is important to know because it'll allow us to understand how we can target treatments.
William Brangham:
And, lastly, in the few seconds we have left, on those treatments, there are some that show some promise on long COVID?
Katelyn Jetelina:
There are.
There's about 300 clinical trials right now, and the results are starting to trickle in. For example, we see metformin, which is a very cheap drug. It reduces long COVID about 40 percent. Paxlovid reduces it a bit as well, maybe about 25 percent. So there is good news on the horizon. But we need more answers.
|
|
|
Long COVID is hot in the news. Does long COVID interest you?
|
|
Yes, but no more than other COVID news.
|
|
|
|
|
Yes, I am concerned or want to know more.
|
|
|
|
|
No. I don't care or think about it.
|
|
|
|
|
|
|
Long COVID: Incidence, Impacts, And Implications
Editor's Note
This article is part of a Health Affairs Forefront series titled “New Challenges for Health Care.” The series of five articles focuses on emerging issues that are facing decision-makers at provider organizations, insurers, public agencies, purchasers, and academic institutions in the health care sector. The articles are written by faculty members at the Icahn School of Medicine at Mount Sinai in New York City, a leading research medical school, and the series is supported by Icahn Mount Sinai.
At his 2023 State of the Union address in February, President Joe Biden announced to the American people that “COVID no longer controls our lives.” Paired with federal government plans to end the COVID-19 public health emergency declaration on May 11, 2023, we find ourselves at a pivotal moment in navigating care for those who have experienced long-term damage from a SARS-CoV-2 infection.
Long COVID remains a significant, long-term consequence of even mild SARS-CoV-2 infections—one with no effective treatments. According to the Centers for Disease Control and Prevention (CDC), as many as one in five US adults who have survived a SARS-CoV-2 infection are still living with the symptoms of Long COVID, and while numbers may vary even conservative estimates place the risk at just below 10 percent. The implications of these findings are that anywhere from 16 to 34 million Americans may be currently trying to navigate life with Long COVID, which will have vast and far-reaching effects on the country. For example, a recent Brookings Institution report highlighted that up to four million working-age Americans are currently unable to work due to the severity of their Long COVID symptoms.
The reality of the current public health situation is that this now-endemic virus has the capability to indiscriminately and perhaps permanently disable up to 20 percent of the people it infects (Long COVID is now a recognized disability under the Americans with Disabilities Act, Section 504). As such, it is incumbent upon us to view this as an emergency situation, regardless of whether the federal government continues to declare COVID-19 a public health emergency or not. In this article, we will aim to fully inform the reader on the emerging literature and landscape around Long COVID, which will hopefully provide context for evidence-informed policy decisions that can limit the impact of this devastating post-viral condition.
How Common Is Long COVID, Who Is At Risk, And What Is The Prognosis?
The overall risk that an acute SARS-CoV-2 infection will result in a Long COVID diagnosis is still hard to pin down as our understanding of Long COVID continues to evolve. A recent review of the available literature estimated that 10–30 percent of non-hospitalized cases, 50–70 percent of hospitalized cases, and 10–12 percent of vaccinated cases of COVID-19 will result in Long COVID.
To date, it has been difficult to identify if there are factors that increase the risk of Long COVID in those who contract the virus. At this time, it is most prudent to assume that anyone who is infected with SARS-CoV-2 has a risk of going on to develop Long COVID. As such, the best available strategy to preventing Long COVID is to prevent the spread of SARS-CoV-2 infection. Unfortunately, this strategy is currently at odds with US public health policy, as the US attempts to “move on” from the pandemic. It remains the responsibility of clinicians and researchers who are working to manage the risk and effects of Long COVID to remind the public that death is not the only serious and permanent outcome that can occur as a result of COVID-19.
To this end, studies that aim to explore the prognosis of Long COVID have yielded little good news. Although one widely publicized recent study analyzing electronic health record data showed that most symptoms of Long COVID resolve within one year, the study suffered from many serious limitations. A recent study that carefully and completely characterized participants with Long COVID showed that more than one-third of the participants reported no improvement in their symptoms 22 months after their initial infection, and only 9 percent reported feeling healthy at the end of the study.
At this stage, with such an incomplete understanding of the underlying causes of Long COVID, it appears overly optimistic to assume that patients will spontaneously recover over time. To understand the underlying causes of Long COVID, it is essential that we work to first understand the different subtypes of the condition.
Treatment And Management Of Syndromic Long COVID
There are currently no well-conducted interventional clinical trials showing success in producing complete remission of Long COVID symptoms. Useful symptom management guidelines have been published by medical societies as well as other allied health associations, and there is emerging evidence to suggest that interventional strategies such as parasympathetic breathing, autonomic rehabilitation, and use of antihistamine medications can significantly decrease symptom burden in people with Long COVID. If there is one important, emerging truth regarding the medical management of Long COVID, it is that treating complex chronic illness requires a highly engaged, interdisciplinary approach. People with Long COVID do not only require multispecialty care, but it is crucial that all involved specialists are in frequent communication with each other to ensure that care plans are aligned and the burden is not on the patient to identify inconsistencies in approach.
It should also be acknowledged that many patients (roughly half) with a Long COVID diagnosis will meet the diagnostic criteria for ME/CFS, and there is much that we can learn from this engaged community of patients. Unfortunately, due to a history of poorly conducted science and medicine’s habit of psychologizing and metaphorizing poorly understood conditions, people diagnosed with ME/CFS prior to the COVID-19 pandemic have endured a legacy of abuse and medical gaslighting when interacting with the health care system. To move forward productively in our ability to treat Long COVID and other PAIS, we must acknowledge the errors of the past and learn from them to re-establish trust with the majority of patients who have experienced harm from stigma associated with their diagnosis.
The Path Forward
As we enter the fourth year of the pandemic, the millions of people now living with Long COVID remain one of the most indelible reminders that the COVID-19 pandemic will continue to be an uncontrolled emergency until we have targeted therapeutics to treat the severe disability that can be caused by SARS-CoV-2 infection. This is an inconvenient truth for those who wish to return to their pre-pandemic lives, but it remains a truth, nonetheless. Scientifically, an optimal path forward will consist of well-conducted longitudinal studies that serve to expertly characterize patients into different subtypes of Long COVID and identify associated biomarkers. In addition, we must invest in high-quality randomized controlled trials of therapeutics such as antivirals, immunotherapies, supplement discovery, and multiple drug combinations to target some of the proven physiological abnormalities already seen in people with Long COVID. They are not served by outdated, debunked, and intellectually lazy attempts to minimize or psychologize what is clearly an aggressive, infection-triggered disease process. As such, research spending on exercise-based therapies or psychological interventions with weak physiological rationales for potential mechanisms of action are wasteful and counterproductive.
We are at an inflection point in our understanding of PAIS, and we have an opportunity over the next few years to conduct research that can drastically change the lives of millions living with Long COVID for the better. Our moral responsibility to our patients with Long COVID, ME/CFS, and other complex chronic illness must no longer be ignored.
|
|
The antiviral drug Paxlovid reduces the risk of getting long COVID
It’s not a panacea, but it might be one of the things that can help
The antiviral medication Paxlovid seems to reduce the chance of developing long COVID, researchers report.
In a large study of veterans’ medical records, Paxlovid lowered a person’s chance of landing in the hospital or dying from all causes in the six months following a COVID-19 infection. And the drug reduced the risk of developing 10 of 13 long-term health problems, researchers report March 23 in JAMA Internal Medicine. On average, the drug lowered the relative risk of developing the conditions by 26 percent, says Ziyad Al-Aly, a clinical epidemiologist at Washington University School of Medicine in St. Louis.
The antiviral drug provided protection against some heart problems, blood clots, kidney damage, muscle pain, fatigue, shortness of breath and two neurological conditions. But it did not lessen the chance of developing liver disease, cough or of getting diabetes after a COVID infection (SN: 1/4/22).
Paxlovid, made by the pharmaceutical company Pfizer, has previously been shown to reduce the chance that susceptible people will be hospitalized or die from COVID (SN: 1/11/22)). To assess the drug’s longer-term effects, Al-Aly and colleagues examined medical records from the U.S. Department of Veterans Affairs’ health care system. The researchers found more than 280,000 patients who had a positive COVID test in 2022 and at least one risk factor for developing severe illness. Of those people, nearly 36,000 got Paxlovid within five days of their positive test result.
The team then compared the health outcomes of those who took Paxlovid with those who did not. Since omicron and its subvariants were circulating in 2022, the researchers compared people in the Paxlovid group only with people in the untreated group who were infected at the same time and in the same geographic region, Al-Aly says. Paxlovid takers had a reduced risk of post-COVID conditions regardless of whether the infection was their first or if they’d had prior bouts with earlier variants. The drug also lowered long COVID risk for unvaccinated people, for those who were vaccinated with one or two doses, and for people who had at least one booster shot.
Some researchers dispute whether the study fully captures what long COVID is. The condition is notoriously hard to define (SN: 7/29/22). “Even in research studies in which we have hours to ask questions, figuring out who has long COVID and who does not is challenging,” says Steven Deeks, a long COVID researcher at the University of California, San Francisco. “These electronic medical record reviews are helpful, but they lack specificity for long COVID. They are great for studying other long-term consequences [of COVID], including cardiovascular events and strokes.”
For instance, many people with long COVID experience post-exertional malaise, or extreme tiredness after exercise, says Monica Verduzco-Gutierrez, director of the post-COVID recovery clinic at the University of Texas Health Science Center at San Antonio. But there isn’t a medical code for that condition, she says, “so it’s hard to pull out of a medical record review.”
Still, the study was able to identify some of the conditions that affect many people with long COVID, including dysautonomia, a condition in which the nervous system has trouble regulating heart rate, blood pressure and breathing.
And the large number of people in the study allows researchers to see effects they might not be able to uncover in smaller randomized control trials, Deeks says. “You can overcome bad data with huge numbers,” he says. In such large studies, “when you do see something, it tends to be real.”
One limitation of the study is that most patients in the Veterans Affairs system are white males, whereas long COVID patients tend to be female, says Al-Aly, who is also the chief of research and development at the VA St. Louis health care system. But he defends the study’s relevance to multiple populations. The study has “literally tens of thousands of women,” he says. “Is it true that the majority are male? It’s true, but you cannot deny the experience of tens of thousands of people just because they’re the minority.”
Paxlovid — as well as other antiviral drugs, vaccination and perhaps a diabetes drug called metformin — might all help protect against long COVID, but plenty of patients who have taken Paxlovid are still showing up in long COVID clinics (SN: 10/24/22).
“We know it’s not this panacea. It’s not going to be a miracle cure for long COVID,” Verduzco-Gutierrez says. “It may be one of the things that can help, or that can decrease the risk, but it’s not going to take it away completely.”
To view the full article, click Paxlovid
|
|
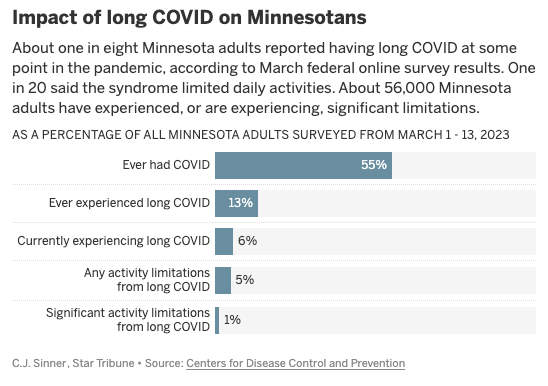
Minnesota organizes long COVID response as pandemic trends improve
Prevalence might be declining, according to federal survey data, but long COVID is still causing substantial and prolonged disabilities in Minnesotans.
Minnesota is organizing its response to the still-mysterious toll of long COVID amid stable or declining levels of the infectious disease this spring.
Twenty doctors and other caregivers are forming a guiding council to study and advise Minnesota on the most effective treatments for long COVID — a cascade of lingering symptoms or health problems following infections with the SARS-CoV-2 coronavirus.
"We still have a lot to learn about long COVID," said Dr. Ruth Lynfield, state epidemiologist and medical director for the Minnesota Department of Health. "But laying the groundwork to expand awareness about the emerging evidence and the available treatments is an important first step toward improving outcomes."
The U.S. definition of long COVID, or post-acute COVID-19 syndrome, is symptoms that linger or re-emerge four weeks after infection. Fatigue and cognitive problems, especially after exertion or exercise, are common symptoms, along with headaches and dizziness.
Minnesota also is launching two surveys to pinpoint the prevalence and severity of long COVID in the state, but an experimental federal online survey suggests it is a common problem. More than 55% of Minnesota respondents in mid-March said they have had COVID-19 at some point and more than 13% reported experiencing long COVID.
Monthly survey results suggest a declining prevalence; nearly 6% of adults reported they were experiencing long COVID in March, down from about 10% in October. Confidence intervals in the surveys suggest the difference could be random chance, but it matches the trend of declining pandemic severity.
Minnesota's weekly pandemic update showed that only 230 inpatient hospital beds in the state were filled with COVID-19 cases on Tuesday, including 18 patients requiring intensive care. That compares to a recent peak of 633 COVID-19 hospitalizations in Minnesota on Dec. 7, and the pandemic record of 1,864 hospitalizations on Nov. 29, 2020.
Duluth-based Essentia Health reacted to the trends Thursday with a switch from required mask-wearing in its northern Minnesota hospitals and clinics to a voluntary stance.
Minnesota is still averaging five to seven COVID-19 deaths per day, reaching a pandemic toll of 14,584 deaths, according to Thursday's update. Death rates have declined among all age groups over the past year, but not as much for seniors — who make up more than 90% of Minnesota's COVID-19 deaths in 2023.
Long COVID consequences are an additional concern. Among Minnesotans dealing with long COVID in March, 83% reported some limitations on usual activities and 23% reported significant limitations, according to the federal survey.
Sampling of coronavirus material in sewage, which has proven an accurate predictor of future COVID-19 illness trends, has revealed declining levels in the state since February.
Viral levels at the Metropolitan Wastewater Treatment Plant in St. Paul had declined 61% over the past four weeks. However, the latest statewide readings through March 22 showed slight increases in fringe metro areas and southeast Minnesota, and a substantial increase in south-central Minnesota.
Recent research from the U's Midwest Antiviral Drug Discovery Center offered another reason for caution: emerging coronavirus variants that are resistant to two antiviral drugs including Paxlovid. The drug became widely available in the U.S. last year and is credited with helping to drive down severe COVID-19 rates.
U researchers said their findings underscore the need for continued development of more drugs with different mechanisms for attacking the coronavirus.
|
|
CDC COVID Data Tracker - March 31, 2023
To get today's break down of positive case data, demographics information, vaccine status and more for Los Alamos County or other counties across the United States, click HERE
|
|
NMDOH Epidemiology Reports - Daily and Weekly Data
As part of the COVID-19 pandemic response, NMDOH collects and analyzes statewide data for COVID-19 positive cases, hospitalizations, and deaths. The reports reflect these critical data and are updated weekly - click HERE
|
|
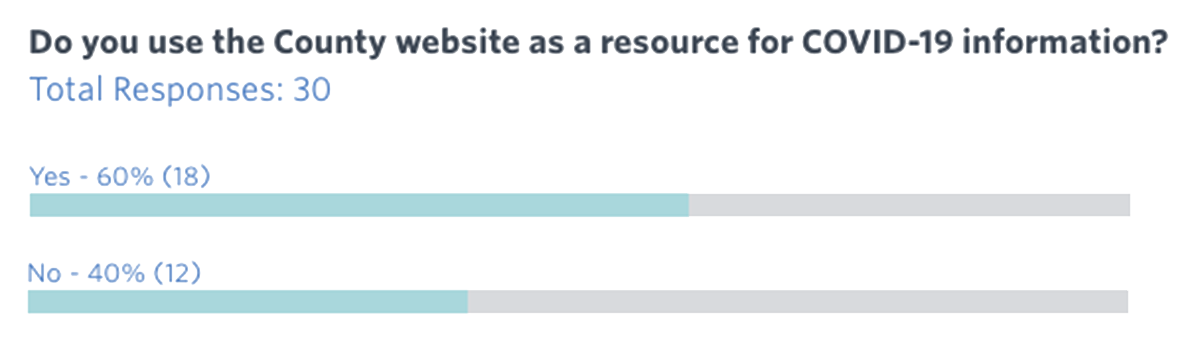
We are listening to you!
Your feedback is helping to shape future newsletters, inform decisions regarding services, and make Los Alamos County healthier and safer. Make sure to participate each week to be heard!
Check out the responses to our last survey:
|
|
Remember, we appreciate your questions! We always try to respond in a timely manner, and if appropriate, we will include those Q&As in future newsletters.
|
|
Have a question? Email us. |
|
Los Alamos Testing Information |
|
The New Mexico Department of Health recommends residents to take advantage of two programs offering free at-home antigen tests, while supplies are available:
-
All U.S. households can order a total of four at-home COVID-19 tests that will be mailed directly to them for free. Tests can be ordered from www.COVID.gov/tests.
-
Additionally, New Mexico residents can receive free at-home tests through the Rockefeller Foundation’s Project Act program while supplies last at: https://accesscovidtests.org/.
Users can follow up with a PCR test from a medical provider or test site to verify results. Visit findatestnm.org to find a convenient location. Individuals can self-report a positive COVID test at Make My Test Count. The reporting of tests on this site is confidential and no personal information is required to use the site.
It is still important to stay home if you have symptoms to prevent the spread of COVID and other respiratory illnesses such as RSV and flu.
|
|
Los Alamos County COVID Testing Resources
Visit the County COVID Page for information regarding testing, click below:
|
|
Los Alamos Treatment Information |
|
Los Alamos County COVID Treatment Resources
Visit the County COVID Page for information regarding treatments, click below:
|
|
Click below to email us your feedback and questions! |
|
|
|
|
|
|