It’s easy to confuse strength of feeling for strength of argument.
The truth is blindingly obvious but convictions can be so much more persuasive.
The NHS is somehow stuck in the middle of what is obvious and what is utility. Can't do what it needs to do because it can't escape from what is necessary.
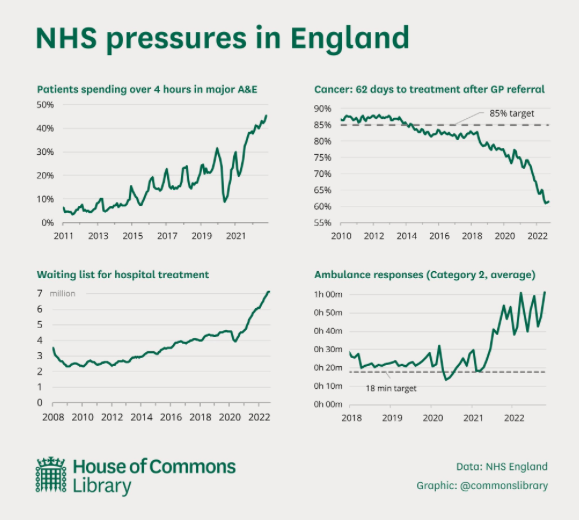
The predicament is; overwhelming demand outstripping capacity.
There's a backlog of around seven million patients waiting for something or other. All of the imperatives point towards getting the numbers down.
The politics, the press, the patients and their families. They all say the same; get the numbers down.
Such as it is able. Such as it is within its power… the NHS will bust-a-gut to do just that. But...
... in normal times, each year, the NHS carries out about 10m operations. Two million are emergencies and the rest are exploratory or elective.
You can see where this is going. Demand is not going away.
‘… the long-term, average number of ‘customers’ in a stationary system (queue) is equal to the long-term average… arrival rate… multiplied by the average time that a ‘customer’ spends (queueing) in the system…’
Normal queue theory tells us dealing with people in the order of their arrival is a golden rule. There is also an assumption, capacity is a constant or a measurable variable.
In the NHS the complexity of team management, rota distribution, staffing gaps and physical resource, cannot guarantee that.
And...
... the practicalities of sickness and trauma, tells us prioritisation is inevitable. Variations in complexity of conditions and multi-morbidity makes a first-come-first-served solution impossible to sustain.
Cancer, if control of the disease is lost, the patient can be lost. Prioritisation of resource, for cancer, is a given.
Varicose-veins, a lower priority for the health system but painful for the patient, whose job may be in a shop, on a production-line or a in warehouse and for whom there will be no greater priority than getting back to work.
No matter how much the likes of Bully-Boy huff-n-puff and the front pages of the tabloids scream, there is not a solution to the demand-versus-present-capacity conundrum.
It will compound.
Improvements in productivity, innovation, cunning plans and culling waiting lists will only work at the margins.
There is no solution… or is there…
There is. It’s not instant and it’s stuck because, we confuse strength of feeling for strength of argument.
It’s blindingly obvious but convictions are more persuasive. Stuck in the middle of what is obvious and what is utility.
The obvious answer is, stop people getting sick in the first place. To do that we need to utilise our data.
The WHO estimate 60% of presentations into healthcare systems are lifestyle related.
This does not mean you all have to join a gym and stop eating chips.
It does mean we have to get smarter at figuring out what makes people sick.
The answer is obvious and available and in our data, notes and history, over which so many people have convictions and arguments about its utility and access.
Each of us has a lifetime of data about when we were sick, what with and what fixed us up.
However, our personal data is useless.
Your family’s data might be more valuable but all our data taken together is a treasure trove. A compass, a direction finder to reducing demand.
Our personal data, which some people have such strong convictions about granting access to.
Our personal data, arguments over which make it impossible to routinely unpick, unpack and use, means the NHS is stranded in a no-mans'-land of the obvious.
There are over 1.3m people who freely, give their blood to save lives, make people healthy and make so much of the NHS possible.
There are over 5,000 people a year who freely donate their organs to make miracles possible.
How many would freely, offer their data to save lives, make people healthy and make a lot of the work of the NHS unnecessary.
People who would say; please crunch my data to help stop the NHS getting crushed.
>> I'm hearing - practice-level appointments data due out this week might be delayed as Digital need to do more work on the data. I wonder what that means?
>> I'm hearing - Greater Manchester Mental Health FT placed in special measures after the scandal of Edendfield was revealed by the BBC. Why the Board is still in place is beyond me.
>> I'm hearing - The RCN have a self funded strike fund of £50m. I'd guess it's because during Covid they collected members subscriptions but didn't have much like events and so-on, to spend it on? I think I'm right in saying their constitution allows them to reimburse strikers up to £7.
>> I'm hearing - from a reader who would like to do a sponsored walk between the 40 new hospitals. Does anybody have the addresses?
>> I'm hearing - last weekend the RCN gave HMG a five day ultimatum to enter 'meaningful talks'. Time's up and they haven't. The College are now boxed in. They'll have to announce strike dates in the next couple of days.