Newsletter of the Alliance's EPIC Learning Health System | | Misfits: Reporting and evaluation in HP | |
Midwifery: Advancing Collaboration in Care
| |
"Kintegration" in Primary Health Care | | New Community Initiatives Data Tool | | Tools to support your IPCT Expansion | | Learning Events
& Programs | | Get Involved: Research & Sharing | | |
Round Peg in a Square Hole:
Misfit between reporting requirements and evaluation practice in community health promotion
Dr. Julia Fursova. University of New Brunswick, and Gillian Kranias, Transform Practice Cooperative
| | |
Have you ever felt that you didn't quite fit in? Like when everything that matters and is unique about you must be tucked away and hidden? Or when you are invited to tell your story, the questions being asked are not central to your story at all? This may be the case with reporting and evaluation for many community health centres as non-profit organizations devoted to community development, health promotion, and social justice.
Our new research paper Round Peg in a Square Hole explores what can happen when reporting and evaluation overemphasize a funder’s functional requirements - to the detriment of community priorities, organizational values, and professional standards.
| | |
Examining the Impact of Reporting Requirements
Our research started in 2017, after many years of front-line health promotion work in community health centres. We wanted to understand how health promotion practitioners navigate the apparent "misfit" between accountabilities that drive reporting and evaluation, what community members valued, and what our professional training and associations teach as vital. This community-based research was informed by our experience as health promoters. Managers, frontline staff and community volunteers from two community health centres engaged with us in shaping and guiding the research project.
Together, we examined reporting requirements for community health centres, exploring how they may influence evaluation methodology choices in a CHCs’ community development and health promotion programs. We were curious to know: To what extent do program evaluation approaches reflect the core principles of health promotion (community participation, interdisciplinarity, empowerment of individuals and communities, and appropriateness to context)?
| | |
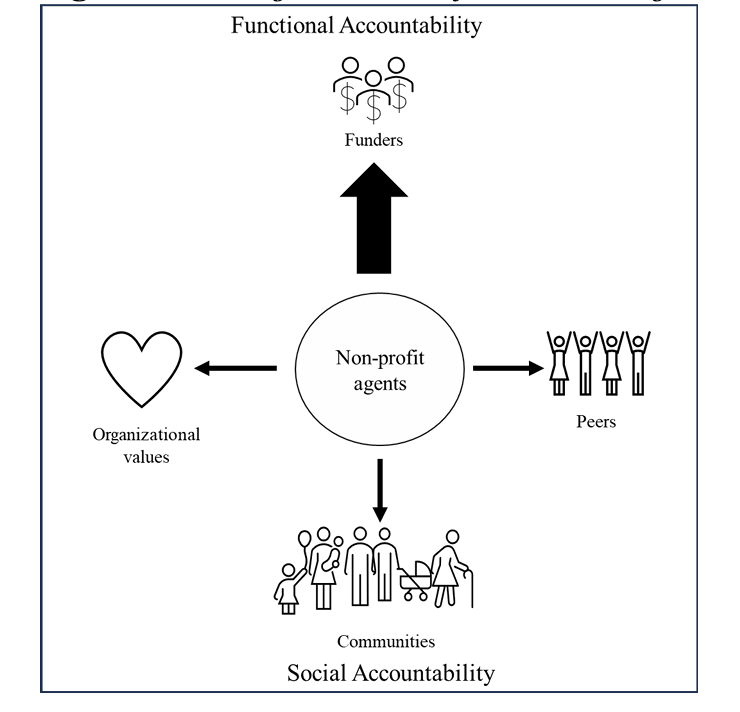
We learned in detail how funder-driven bias in the CHCs’ reporting requirements undermines these non-profits’ accountability to other constituencies, most notably the communities they serve.
These reporting requirements were strictly functional, emphasized efficient service delivery, and failed to ask adequate questions for capturing the outputs of community development and health promotion programs - let alone their impacts.
| |  | Figure 1 Existing Directions of Accountability in the Non-Profit Sector and Their Funder Bias. Click image to access larger version with Alt text. | | |
Finding a Knot
By analysing the relationships among reporting requirements, evaluation activities, and program design, we discovered a knot of three entangled tendencies:
- A clinical model and biomedical view of health embedded in the structure of reporting requirements.
-
Methodological pressures and capacity constraints for health promotion evaluation.
- A weakened community participation in evaluation.
These three phenomena, and the effects they produce, surface in a visual mixed media collage entitled “Reporting and Evaluation Puzzle in Health Promotion”, by Julia Fursova (Figure 2, below). The collage-making is part of Julia’s methodology of data analysis and visualization.
In the collage, a vintage typewriter represents the reporting requirements - “the machine” of funder-driven accountability systems (driven by neoliberal economics) that ask a perpetual question, “how much money did you spend?” Meanwhile, stories about the dynamics and impacts of community development and health promotion programs, represented by everyday items such as teabags and buttons, float around near the bottom corner of the collage. They remain distant from the numbers and invisible to the accountability system. These diverse stories, voices, and knowledges find no pathway into the organization’s evaluation and strategic learning system.
| | Figure 2: "Reporting and Evaluation Puzzle in Health Promotion." Mixed media collage by Julia Fursova. Click image to access larger version with Alt text. | | | |
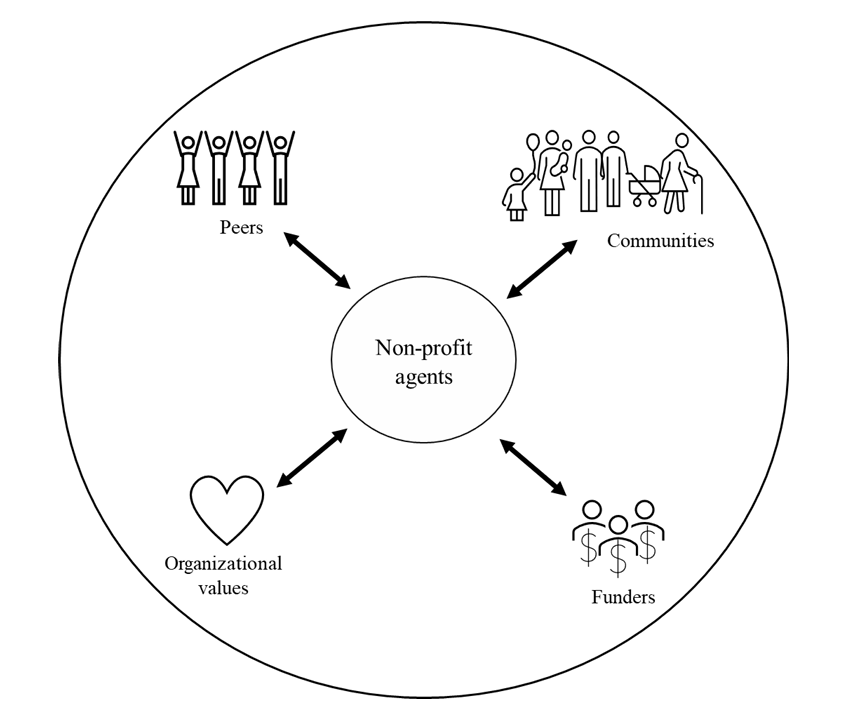
To untangle this health promotion evaluation ‘knot’ - of clinical model, methodological pressures, and undermined community participation - we propose a “wholistic accountability system”.
This model shifts funder-oriented functional accountability interests away from the “top” and brings the position of the funder into balance with those of the community, organizational values, and peer accountability (see figure 3).
| | | Figure 3 Circular Framework for a Wholistic Accountability System. Click image to access larger version with Alt text. | | Julia Fursova, PhD (She/They), School of Leadership Studies, UNB, is an academic partner, co-director, and co-founder with Transform Practice not-for-profit co-op. Julia is a community-engaged scholar whose research program has been influenced by their lived experience as an immigrant, continuous dialogue with community members and a commitment to anti-oppression and decolonization in research and action. Julia’s previous roles in CHCs include community engagement worker (Lawrence Heights CHC, Toronto), health promoter and case coordinator (Unison HCS, Toronto), and Guys Can Cook! Project Co-ordinator (Four Villages CHC, Toronto). Most recently, Julia worked as a consultant supporting a participatory evaluation of Black-Focused Social Prescribing program with CHCs. | Gillian Kranias (They/She) has contributed to dozens of equity-centered community development, community planning, and systems change initiatives. Each was stronger from investments in collaborative, creative, and participatory evaluative learning activities. Gillian is proud author of two practical, accessible resources on participatory evaluation: The Power of Reflection, and Participatory Evaluation Toolkit. Gillian’s foundations are an MES in Community-based Organizing for Environmental and Social Change and over three decades of ‘learning through action’ alongside powerful leaders from diverse equity-seeking communities. Today, they contribute to change as a co-director with Transform Practice Cooperative and as Manager, Learning and Evaluation at the Canadian Women’s Foundation. | | |
Better Care for Early Pregnancy Loss
A Collaborative Approach Between Community and Hospital with Midwifery Leadership
Shezeen Suleman, RM, and Jenna Bly, RM, MATCH Program, South Riverdale
| | |
The poor quality of care for early pregnancy loss (EPL) in Canada has been a frequent topic of conversation across the country since the Canadian Medical Association Journal published this article flagging the issue last year. A unique collaborative model between midwives and obstetricians at Michael Garron Hospital’s Early Pregnancy Clinic (EPC) has been addressing these gaps in EPL care head on.
Although midwifery has been regulated and publicly funded in Ontario for more than 30 years, until very recently, midwives have only provided care for families who are able to and chose to carry pregnancies to term. But the midwifery model of care, which is distinguished by its collaborative, patient-centred approach, has the potential to offer high quality care for all pregnancies, regardless of outcome. This potential was highlighted in this recent article in the journal Sexual and Reproductive Health Matters.
| | |
Introducing MATCH: A new collaboration begins
The Midwifery and Toronto Community Health (MATCH) Program is a full-spectrum perinatal care program that has been operating at the South Riverdale Community Health Centre in Toronto since 2018. In 2021-22, Ontario’s Ministry of Health approved expansion funding for MATCH. With this expansion, MATCH midwives began staffing Michael Garron Hospital's EPC in 2023 with the goals of improving patient experience, reducing wait times, and improving follow-up care.
Since assuming co-leadership of the EPC, the midwives have been able to increase access to the clinic and have worked towards improving quality of care by leading the development of evidence-based approaches to care now shared across the unit. An interprofessional hospital-community partnership like the one at the MGH Early Pregnancy Clinic is unique in Canada, maximizing the scope of practice of midwives and obstetricians while improving patient care.
| | |
Improving access, care, and experience
In less than two years of midwifery staffing of MGH’s Early Pregnancy Clinic, midwives from SRCHC have made improvements towards the quality and safety of early pregnancy care in the clinic, the hospital, and the community.
- They have developed evidence-based protocols in collaboration with their obstetric colleagues to standardize practice across a large, interprofessional team.
- They strengthened relationships between the Departments of Midwifery and Obstetrics through regular working group meetings, feedback pathways, rounds, and collaborative, team-based care.
- They provide education for primary care providers and community midwives related to the management of early pregnancy loss.
- They have created patient handouts specific to the clinic, designed for the community and making them available through the hospital website.
Additionally, they’ve improved the accessibility of early pregnancy care for community members, by:
-
Expanding clinic hours from 2 days a week to 4 days a week.
- Establishing a 7-day-a-week phone line for patients to ask clinical questions and receive a response from a midwife within 24 hours.
- Working with hospital leadership to establish a pathway for uninsured patients to receive free, hospital-based care as outpatients.
- Developing an updated referral form and a dedicated webpage for the EPC
-
Improving referral pathways between community and hospital for patients experiencing early pregnancy loss and other complications of the first trimester, such as ectopic pregnancies.
This has resulted in shorter wait times and quicker access to follow-up care. They have also improved access to medication abortion for termination of pregnancy in the hospital setting.
| | |
The MATCH team have also worked with the hospital to make the clinic space safer and more welcoming space for clients experiencing pregnancy loss.
- The clinic is now in a dedicated space with its own entrance and a private waiting room, so patients experiencing grief and loss no longer have to share space with families that have healthy infants.
- They’ve accessed funding for artwork that makes the space inviting, comforting and beautiful.
- They’ve improved signage and wayfinding for those accessing the clinic
| | | |
Demonstrated Potential for Transformation
Canada’s healthcare systems provide ready access to specialist care (obstetricians and midwives) for patients who present with complications in the second and third trimester. Sadly, for those experiencing complications in early pregnancy, the emergency department is often the only option, despite the fact that most of these patients are stable and should be assessed by specialists in an outpatient setting.
Collaborative care models like the one between midwives at South Riverdale Community Health Centre and obstetricians at Michael Garron Hospital have the potential to transform patient experience and improve care for all pregnancies.
| | |
Shezeen Suleman and Jenna Bly are Registered Midwives and co-leads of the MATCH program at South Riverdale Community Health Centre. |
| | |
Kintegration:
Incorporating Exercise into Interprofessional Primary Health Care Teams
The Ontario Kinesiology Association
| | The science is clear: Exercise is one of the most important contributing factors to overall health. However, many people experience barriers to an active lifestyle. By including someone on your interprofessional team, such as a kinesiologist, who can help make physical activity accessible, you can improve health at the individual, community, and population levels. This, in turn, can reduce demand for acute or episodic care in your community. | |
"Kintegration" at Guelph Family Health Team
“Kintegration” at Guelph FHT
At Guelph Family Health Team (GFHT), kinesiologists are helping clients who have or are at risk of developing diabetes to look after their health and wellbeing. GFHT’s interprofessional team includes two Registered Kinesiologists who work in their Diabetes Education Program. They help clients choose and follow exercise plans that first address diabetes and chronic pain, then work outward to improve outcomes for as many comorbidities as possible.
Clients and community members are referred to GFHT’s Diabetes Care Program in two situations:
- Those who are at risk of diabetes or diagnosed with pre-diabetes are referred for primary prevention of diabetes.
- Those with a diagnosis of Type 1 or Type 2 diabetes are referred for diabetes management and education.
Referrals come from a variety of sources. Some come from practitioners within the GFHT itself -- physicians, nurse practitioners, and interprofessional team members, such as dietitians. Others come from providers outside GFHT, such as solo physicians and staff at local community health centres. Kinesiologists within the program build physical activity-based programs that address as many comorbidities as possible, working to improve both diabetes and general health. The two kinesiologists work at different sites, each of which has a gym, and people who access the kinesiologists can use these gym spaces at no cost.
| | |
Kinesiologists in Other Settings
Such an approach can work equally well in a different setting, such as a Community Health Centre. If you are looking for a cost-effective approach to increasing your organization’s capacity for access and attachment, you may wish to consider adding a kinesiologist to your team. Like other health professionals, kinesiologists are classified as Unit Producing Persons (UPPs), whose salaries are funded by the Ontario government. For CHCs that operate as charities, donor and grant-based funding models may also be an option. If you already have a kinesiologist on your team, you may be able to expand their capacity through the use of medical directives or additional certification.
A strong business case can be made for adding a kinesiologist to your interprofessional team or funding them to attain additional certification. According to the Public Health Agency of Canada, exercise has been shown to reduce the risk of more than 25 chronic conditions. These include helping to prevent or manage symptoms of many of the most common ones affecting people in Ontario, including type 2 diabetes, hypertension, depression and anxiety, and COPD. Kinesiologists working to their full scope of practice can make exercise more accessible to clients and community members, provide regular preventive care, improve population health, and ultimately ease the human resources load on other front-line health professionals.
| |
Recording Community Initiatives in the EMR
An Updated Tool to Support Storytelling, Learning, and Quality Improvement
Alliance for Healthier Communities
| | Although they are essential, Community Initiatives are often misunderstood or overlooked by policymakers and funders. In her 2017 report, Ontario’s Auditor General highlighted the importance and uniqueness of CIs but noted that CHCs weren’t consistently tracking information on them. She recommended that CHCs increase their efforts to collect and analyzed data to measure outcomes for all types of services they provided, including CIs. | | A New Approach to Recording Community Initiatives | | |
There are some real challenges facing the documentation of community initiatives. For example, CIs often have no clear beginning or end. They tend to evolve out of ongoing community discussions and existing activities. Partners and participants may come and go, and issues may change over time. Likewise, goals and objectives may shift as work with the community progresses, so outcomes may be different from those originally conceived.
To accommodate these characteristics, the evaluation approach calls for a monthly snapshot of achievements that have occurred during the month under review, as well as lessons learned and numbers of participants. The new CI tool consists of two custom forms for the TELUS PS Suite EMR: A one-time registration form that records the start date, goals, partners, target population, and objectives of each CI, and a monthly activity form which records details about specific activities, including the staff and community partners involved, number of participants, key achievements, and key learnings.
| | |
Implementing the New Tool and Supporting Alliance Members
The new CI tool was released to Alliance members in September 2025. The custom EMR forms were distributed to executive leaders by email and made available for members’ data staff to download from a secure online portal. These forms were accompanied by Community Initiatives Data Entry Manual (also available in French), which describes not only the steps to record CI data but also the rationale and definitions for each data element. The tool was formally launched through a Lunch & Learn webinar and subsequent Q&A session.
Alliance members who want additional support with implementing and using the new tool, or who wish to deepen their understanding of CIs and their data elements are invited to contact Christine Randle, Provincial Data Management Coordinator at the Alliance.
| |
Building a Neighbourhood Health Home
How the Alliance is Supporting IPCT Expansion
Alliance for Healthier Communities
| | Challenges faced over decades by health care organizations have fueled a crisis of access to primary health care. In response, the Ontario Government has granted funding for Interprofessional Primary Care Team (IPCT) expansion to selected organizations across Ontario. The Alliance for Healthier Communities has developed a suite of tools to support good stewardship of this funding and help organizations build capacity in ways that can advance health equity, make care more accessible, and improve population health. These tools are being shared publicly so that primary health care organizations across the province, regardless of model, can benefit from them. | | |
A Neighbourhood Health Home
The Neighbourhood Health Home (NHH) is a model of locally integrated health care, with primary care as its foundation. In this model, a “hub” provides comprehensive, interprofessional care in collaboration with local “spokes.”
| | |
The hub is a community-governed, equity-oriented primary health care organization, and the spokes are a network of local partners in primary care – other teams, fee for service physicians (FHO, FHGs and Solo Practice MDs), and community agencies. Six pillars support and sustain the NHH:
- Interprofessional, collaborative primary health care
- Community governance and engagement
- Population-based approach to health
- A strong data foundation
- A focus on equity and the determinants of health
- Accountability and efficiency
| |
| |
This model is grounded in the Model of Health and Wellbeing and aligned with what Alliance members have been doing for decades: delivering collaborative, person-centred care that supports population health.
The Neighbourhood Health Home model was first shared publicly in April 2025, in a lunch ‘n’ learn webinar. Alliance CEO Sarah Hobbs and Director of Research and Policy Dr. Jennifer Rayner outlined the NHH vision and described its potential to advance health equity and improve the health and wellbeing of people across Ontario.
| |
EOI 2025 Toolkit
This toolkit was developed to support organizations in developing an Expression of Interest (EOI) for Fall 2025 funding that incorporates the Neighbourhood Health Home vision. It provides suggested approaches for completing each of the EOI’s eight sections as well as strategic considerations, links to resources, information about the EOI evaluation criteria, and tips for preparing a budget. A generalized case example with specific references to the NHH and the “Hub and Spoke” model was also created as a companion document to the EOI toolkit.
In October, the Alliance held a webinar on Practical Guidance of IPCT Expansion EOI to further support EOI development. Sarah and Jennifer, along with Kimberley Floyd, Chief Executive Officer at Wellfort CHC, described a living example of the NHH in action, supported by the first round of IPCT expansion funding.
| |
IPCT Expansion Toolkit
The Interprofessional Primary Care Team (IPCT) Expansion Toolkit consists of resources created and collected by the Alliance to support organizations in making the strategic and operational decisions necessary to implement their expansion plans. Originally developed for Alliance members who had received expansion funding, it was shared publicly as a resource for any primary health care organization that seeking to increase their capacity and equitably improve access and attachment to primary health care for people in their communities.
Many of the resources in the toolkit were shared by Alliance member organizations or created with their help. They include case examples, change ideas, and practical tools, organized into nine chapters that address diverse topics such as:
- Optimizing workflow to increase capacity
- Using technology to support operational efficiency
- Data collection and reporting
- Building a connected health neighbourhood to support equitable access
- Developing pathways to primary care attachment for unattached people
Although it has been live on the Alliance website since the spring of 2025, this toolkit was officially launched in a webinar last month. Jennifer Rayner and two of the Alliance’s Quality Improvement & Performance Leads – Stéphanie Lamothe and Denis Tsang – demonstrated how a primary health care decision-maker might use the toolkit to address several expansion-related pain points.
Because the health care landscape is continually evolving, the Alliance will be refreshing and updating the toolkit this fall and winter. After going offline for a few weeks in January, it will be relaunched in early 2026.
| |
Exclusive Supports for Alliance Members
All of the resources listed above have been made available for free to the public. Additional supports are also available to Alliance member organizations. In the summer of 2025, the Alliance launched its fourth learning collaborative, Increasing access through intake process improvements – Using an equity-based approach. Like the Alliance’s other learning collaboratives, it consists of alternating learning sessions and action phases with dedicated QI support and coaching from our Quality Improvement & Performance Leads (QIPLs). In a Capstone event next summer, participating teams will share their projects and learnings. In addition to the learning collaborative, Alliance members who have received IPCT funding are invited to participate in a dedicated Community of Practice to share their experiences and engage in collaborative learning and solution-finding. As always, individualized support from the Alliance’s provincial Data Management Coordinator and QIPLs is also available to Alliance members.
| |
Learning Events & Programs
| | |
Women and Children
Tuesday, January 13, 12:00-1:00 pm | Online | Free
Presented by the Institute of Health Emergencies & Pandemics
| |
Ongoing Training and Collaborative Learning
Echo at UHN
Free, interprofessional, collaborative learning funded by the Ontario Ministry of Health. Join ongoing cohorts on liver, concussion, rheumatology, and chronic pain & opioid stewardship. Register here.
Rapid Action & Learning Intensive on Sociodemographic Data Collection
Free, open to Alliance members only. Sign up any time for access to four online modules, a workbook to help track your progress, and expert coaching support if and when you need it.
SPIDER Learning Collaborative: De-prescribing dangerous medications
A QI approach to de-prescribing potentially harmful medications for medically complex seniors. EMR queries available for participating Alliance members. Contact Jennifer Rayner for details.
The Canadian Social Prescribing Exchange
All individuals and organizations in Canada who are interested in social prescribing are welcome to participate. Presented by the Canadian Social Prescribing Exchange. Register here.
Bamemin – To Care For: Cultural Safety Training for Health Care Practitioners
Free, online cultural safety training from the Ontario Native Women’s Association, developed to improve healthcare delivery for Indigenous women and their families.
| |
Research & Sharing Opportunities
| | |
CPRI Research Symposium 2026
Posters and oral presentations about child and youth mental health, focusing on these two themes:
- Tailoring Dose, Duration, and Frequency for Therapeutic Interventions
- Designing Healthy and Supportive Spaces in a Technological Age
Conference date: June 16, 2026. Submit abstracts here by January 12.
| | Research Participants & Partners | | More Tools for Improvement and Highest-Quality Care | |
Looking for more?
Consider subscribing to these newsletters to receive regular updates from Alliance system partners:
| |
Got a moment?
Tell us what you think of EPIC News
| |
| Do you consider the content relevant? | | | |
| Do you consider the presentation (writing, layout, visual elements) to be engaging? | | | | |
Thank you!
Your responses will help us make EPIC better.
Please send comments, suggestions, or story ideas to LHS@AllianceON.org.
| | | | |