|
When the newspapers put their headline boots on…
… you can be sure someone is heading for a kicking.
Their target right now, is the UK Health Security Agency, pronouncing…
… their response to the recent meningitis cluster was... too slow.
Was it? Let's have a look.
At the centre, it looks rapid and structured; on the ground, it probably looks like running to catch-up.
Both can be true at the same time.
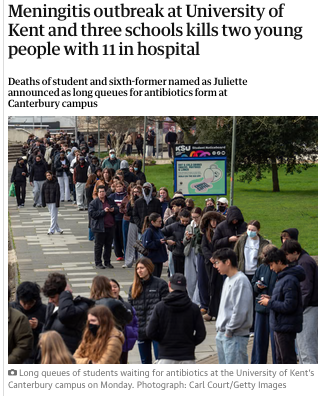
Students fall ill on Friday. Diagnosis confirmed, Saturday...
... by Sunday the machinery moved in the way it is designed to.
Public health teams, led by the UKHSA, began contact tracing, identifying close contacts, and arranging prophylactic antibiotics.
Universities shifted into response mode, issuing advice, adjusting teaching arrangements and supporting students.
On paper, this is a system doing what it should;
- evidence gathered,
- thresholds met,
- actions triggered.
But…
… meningitis is not a disease that tolerates process. It moves quickly, often brutally, and by the time a cluster is confirmed, several people may already be seriously ill and in this case, the worse case possible... they died.
This creates the uncomfortable gap between recognition and reality.
Public health systems are built to avoid false alarms; meningitis punishes hesitation.
The result is a familiar tension…
… act too early and risk panic and overreach…
… act too late and the consequences are measured in lives, not inconvenience.
This is where much of the criticism is fermenting.
Not so much in the clinical response, which appears to me to have been swift, but in communication and escalation.
Families and students understandably ask why warnings did not come sooner, particularly once severe cases emerged.
From their perspective, information is part of the intervention.
From the system’s perspective, information is calibrated, verified and targeted.
The two don’t align, and...
... let's not forget, the role of the university.
Universities are not responsible for diagnosing cases, prescribing antibiotics, or determining who counts as a close contact. That sits firmly with public health authorities, but…
… universities do carry a duty of care. Once they know, or reasonably ought to know, that there is a credible risk, they’re expected to act;
- to inform students,
- provide clear advice, and
- support access to care.
There are two parallel responsibilities.
Public health decides who needs treatment.
Uni’s decide how their wider community is informed and supported.
However, when the question shifts from informing students to informing parents, the ground changes completely.
In UK law and clinical practice, once a student is 18, they are an adult patient, meaning…
… their medical information is protected by strict confidentiality rules.
Neither the NHS nor the university has a general duty, or even the legal right to inform parents that their son or daughter has been hospitalised, unless…
… the student has given consent.
This sounds counterintuitive, particularly in acute and frightening circumstances, but it reflects a fundamental principle…
… the duty is to the patient, not the family.
There are exceptions. If a student is unconscious or lacks capacity, clinicians may act in their best interests, which can include contacting next of kin.
In many cases, students themselves will ask for their parents to be informed, or will have provided emergency contact details that can be used appropriately, but…
… there is no automatic parental entitlement to information, even in serious illness.
Uni's position gets worse. They’re not part of the clinical-care team and cannot disclose personal health information about a student without consent.
Even confirming that a student is unwell may breach confidentiality.
What they can do is encourage students to contact their families, support them in doing so, and communicate general information to the wider student body.
This is where expectation and reality collide.
In a crisis, people assume parents will be told. In practice, adulthood… and the rights that come with it.. get in the way.
If there is a single thread of management thinking running through all this, we must turn to Edwards Deming, who said;
'… every system is perfectly designed to get the results it gets...'
-
Public health waits for evidence;
-
Universities balance duty of care with legal limits;
-
Clinicians prioritise patient autonomy.
The difficulty is that meningitis doesn’t wait, and…
…in that gap between process and pace, everything can feel too slow, even when, technically, it is not, but...
... technicalities mean nothing...
... perception is everything.
|