|
If Tanya had had a couple of hours sleep in the last three days, it would have been a lot.
She looked exhausted.
Clutching her new born, wrapped in a blanket, she struggled out of the chair, along the hallway, to opened the front door.
‘Hello, I’m Alison. I’ve come to see how you’re both getting on….......’
Her voice tailed off, as Tanya burst into tears.
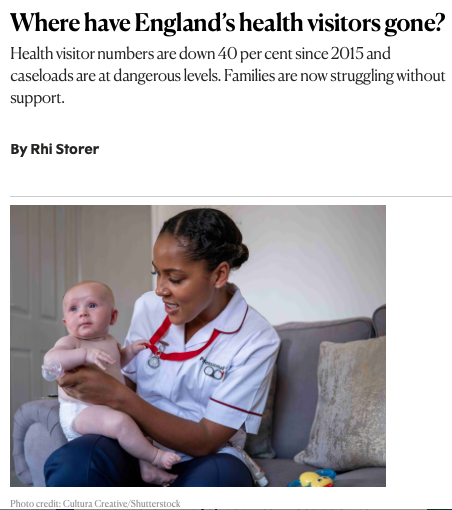
Welcome to the world of the health visitor.
When we talk about pressure in A&E, two groups dominate the data, older people and the under-nines, of which...
... the under ones are the largest group of people by far. The 0–4yrs attending A&E has increased by 42% in the last 10 years.
In North West London, 59% of babies who attended A&E didn't need treatment... sent home after reassurance...
... it costs an estimated £1.8 million.
In different ways, both connect back to the upstream question…
… what’s happened to prevention?
Since 2015, there have been 6.5million live births in England,
and…
… the number of health visitors in England has fallen from around 11,000 to roughly 6,300, call it 40%.
Commissioning moved from the NHS to local authorities, HV funded through the Public Health Grant. Under absurd financial pressure, councils have cut posts, let vacancies run.
Do the maths…
… well over 3.25 million children should be under the care of HVs…
… caseloads should sit around 250 children per HV now frequently run to 500 or more.
... 73% of HVs said; workforce shortages had impacted on their ability to support families when a need was identified,
All this is not just another workforce issue. It changes risk-distribution across the system.
Health visitors deliver the Healthy Child Programme…
- universal contacts from pregnancy to age five,
- developmental reviews,
- safeguarding,
- maternal mental health support,
- immunisation promotion,
- feeding advice
- accident prevention.
If it's a canary in a mine... it's a HV that's the early warning system in the home. When that signal weakens, risks and costs migrate.
A large share of paediatric A&E attendances are for fever, viral infections, rashes, minor head-injury and breathing worries.
International evidence on structured home-visiting programmes shows improved parental-confidence and reduced visits to A&E.
Regular contact builds ‘health literacy’;
- when to worry,
- how to manage symptoms,
- where to seek appropriate help.
If that trusted relationship is absent, anxiety defaults to the only guaranteed 24-hour access point… A&E.
Vaccination is another link in the chain. Health visitors are key, in encouraging uptake.
Following-up families who miss appointments. Lower coverage means outbreaks of preventable disease… like the measles outbreak in London… which will drive emergency demand.
There’s no argument; absent HVs reduce proactive community engagement.
Correlating with lower uptake… which increases avoidable illness.
Safeguarding presents a more serious dimension. Early nurse-led home visiting, shown in multiple studies, reduces child abuse.
HVs can detect subtle risk factors… mum's depression, domestic stress, neglect. A&Es struggle with this.
When caseloads double, time for observation shrinks. Risk will surface… usually in A&E.
Developmental delay is a longer arc. Speech and language problems, concerns about neurodevelopment and behavioural issues are often first identified by HVs.
Without early intervention, difficulties compound.
Over time, the link between adverse childhood experiences (ACE) and adult morbidity becomes clearer.
The ACEs literature consistently demonstrates associations between early trauma and higher lifetime rates of cardiovascular disease, diabetes, respiratory illness and mental health disorders…
… the very conditions that dominate emergency admissions among older adults.
Early-year’s workforce doesn’t only influence paediatric A&E. It shapes the health trajectory of the next generation of older patients.
Families don’t stop needing support when HV support stops.
Demand shifts downstream, care substituted…
- first to general practice,
- then to urgent care,
- then to A&E…
… emergency departments become the system’s shock absorber.
It’s called failure demand… demand and costs created elsewhere because it’s not met where is should be met.
Health visiting is not the sole driver of paediatric attendances. Deprivation, primary-care access and parental employment patterns all play roles, but…
… removing more than 4,000 specialist public-health nurses from the early years landscape removes a protective factor at population scale.
There’s a symmetry. Probably a contradiction. We invest heavily in urgent treatment centres, triage algorithms and flow management to reduce avoidable A&E use. Yet, we’ve allowed the preventive structure of early childhood to crumble.
Managing consequences while trimming causes.
Serious about reducing A&E pressure? Forget operational reform inside hospitals. Sort out structural reinvestment outside.
The decline of health visiting is not just an early-years story. It is part of the causal-chain that runs, slowly and predictably, from…
… the front door of a new-born’s home, right to A&E's front door.
|