|
Join Our List
 |
|
Robin Novak, RN, CIC
|
 |
|
Director of Infection Prevention
and
Endoscopy
636.875.5088 ext. 101
|
|
This Month's Training Opportunities
|
 |
None for December
Coming in January:
"WISH: Wash-IUSS-Sterilization-HLD"
Several new Infection Prevention titles added this month.
|
|
Surveyor's Corner
|
 |
|
Cathy Montgomery, RN, CASC
AAAASF Surveyor
636.875.5088 ext 102
A very perplexing situation exists at many ASC's when it comes to holes, perforations, tears in vinyl/leather coverings. This frequently involves mattresses, foot pedals, pillows, etc. Common practice is to try to cover the area with surgical tape; this will result in an automatic citation if discovered. This is one of the first places I check while doing a survey or mock survey.
Once you have a breach in your covering, it becomes impossible to clean and you have no assurance your efforts will be successful at removing any sources of bacteria etc. This is why the surgical tape does not work; it does not properly cover the area, nor can it in and of itself be cleaned along the surfaces satisfactorily.
For single small areas I have had great success with CleanPatch, which is FDA approved if used properly. For larger areas, folds, or corners you are looking at replacement or recovering. Two pieces of advice:
- If you choose to recover, make sure your product is sturdy and you obtain the manufacturer's recommendation for cleaning products.
- Which brings me to cleaning products! This may actually be the initial cause of your tear as you perhaps did not look at labels to see if what you are using is appropriate for your leather /vinyl in the first place. Turns out your efforts to destroy germs are too harsh for your cover.
|
|
Recent Events
|
|
CMS has finalized the quality reporting protocols for 2017. For 2017, there are no additional quality data measures. You can find the specification manual at
QualityNet.org.
If you missed our training classes on implementation strategies,
CLICK HERE to learn more or purchase view-upon-demand.
However, the 2018 quality measures will include several additions. Measurements will include: 1) unplanned anterior vitrectomy, 2) normothermia and 3) several portions of the OAS CAHPS Survey. You can read about it in the Federal Register or again, see our view-upon-demand presentation. Ambulatory surgical centers begins on page 79732 of F.R.
NHSN has updated the Surgical Site Infection (SSI) Event module. You can find it at:
|
|
|
|
Volume 1, Number 2
|
December 2016
|
 |
This is the second month of the rebirth of our Infection Prevention Newsletter and at the same time introduce our new Director of Infection Prevention, Robin Novak, RN, CIC!
Our newsletter has been appropriately renamed
ImPaCT and the goal is to offer monthly discussions by Robin on the infection prevention and control trends for ambulatory surgery centers.
ABOUT ROBIN NOVAK, RN, CIC
Registered Nurse, Certified Infection Preventionist dedicated to disease prevention and high quality healthcare. Strong decision maker who understands the importance of patient, visitor and staff safety following evidence based best practices.
Driven and compassionate healthcare professional with 30 years hands-on experience in fast-paced ambulatory surgery center and hospital environments. Accountable and responsible with an additional focus on Quality Assurance Process Improvement
.
In the past, Robin has served as the SGNA Carolina Chapter President, involved in SGNA Practice Committee as well as a Regional Committee member. Robin has been active with APIC and is a current member of APIC PALMETTO. Robin was prior employed at the Ambulatory Surgery Center of Spartanburg since 2004 and held roles of Endoscopy Nurse, Endoscopy Charge Nurse and most recently the Quality Assurance Process Improvement Coordinator. Robin has worked on several infection prevention projects for Excellentia Advisory Group including a key role as a faculty speaker at our annual Infection Prevention Strategies for ASC's conference in Las Vegas.
|
|
ZERO TOLERANCE
|
By Robin O. Novak, RN, CIC
Safe injection practices remain one of the top infection control deficits that surveyors find during audits. As healthcare professionals, this trend should not only alarm you, but it should awaken your passion and commitment to always do the right thing. Our patients safety and lives depend on it.
What makes an injection unsafe? There are a variety of errors which can contribute to adverse patient outcomes.
1)
Using a vial which is labeled as single use more than one time. A single use vial does not have preservatives; therefore, there are no properties to prevent microbial growth. That means you can only pierce the rubber septum one time after disinfecting it with alcohol.
2)
A multi-dose vial may not be accessed in a patient care area. While this seems impractical, it is another patient safety safeguard. When a multi- dose vial is accessed in a patient care area such as an OR; it increases the risk of contamination of the contents, thus making it dangerous for the next patient.
3)
Syringes and needles may only be used one time. That means only one entry into a vial followed by one entry into the intravenous tubing hub after disinfection with alcohol.
4)
Glucose and hematocrit monitoring units must be identified by the manufacturer
as multi-use. The lancet device must be auto retracting and single use.
Are you interested in learning more? Are you searching for behavior modification ideas? Be sure to check out my view-upon-demand video presentation available at CLICK HERE.
|
| Critter Craze |
By Robin O. Novak, RN, CIC
C. difficile: What is the scoop on the poop?
The prevalence of C. difficile is not a surprise to infection preventionists. Historically, C. difficile was related to recent antibiotic use. It can be one of the leading causes of healthcare-associated infections. What is the scoop on the poop?
Per the CDC, it was estimated in 2011 there were 500,000 C. difficile infections. Of those, approximately 83,000 patients experienced a recurrence, and 29,000 died within 30 days of the initial diagnosis.
Clostridium difficile is a spore-forming, gram-positive anaerobic bacillus. It produces two exotoxins and is a frequent cause of antibiotic-associated diarrhea. Patients at greatest risk for developing C. difficile are those with recent antibiotic exposure, use of proton pump inhibitors, GI surgery/ manipulation, long length of stay in healthcare settings, immune-compromising conditions and advancing age. Patients will present with symptoms of watery diarrhea, fever, loss of appetite, nausea and abdominal pain/ tenderness.
C. difficile is shed in feces. Therefore, any surface which comes into contact with the infected feces becomes a reservoir for the spores. C. difficile spores can live on surfaces for up to five months if not adequately disinfected. Healthcare workers, family members and visitors may then unintentionally pass the C. difficile spore onto others just by touching the contaminated surface.
The number one, best defense against C. difficile transmission is appropriate hand hygiene with soap and water. Since the C. difficile spores are not affected by alcohol-based hand rubs, the performance of hand hygiene using soap and water will wash the spores down the drain.
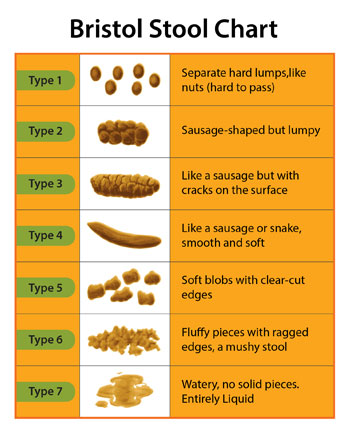
Quick identification of C. difficile may be a limiting factor for the disease. Anytime a patient has unexplained diarrhea; they should be tested for C. difficile. The best test is a stool sample, but it is most often associated with false-positive results. Therefore, it is important that healthcare providers are acutely aware of the types of stools which qualify for testing. The use of the Bristol stool chart can be beneficial in identification. Remember, it has to be type 7 to be tested.
|
| GI Corner |

By Robin O. Novak, RN, CIC
What's your story? Endoscope transport!
Transport of endoscopes is becoming a topic of concern in the GI community. Questions remain as to how facilities are meeting the requirements. As you are aware, every endoscopy unit is different, and each has its'set of challenges.
The requirements for endoscope transport are found in the three main endoscope reprocessing guidelines: AAMI, AORN, and SGNA. Although each offers a slightly different approach, they are all similar. A contaminated endoscope must always be transported in a container which provides the following characteristics: a) labeled with biohazard label b) have a lid c) be puncture resistant. The rationale is to protect GI healthcare workers from potential bloodborne pathogen exposure. Keeping that in mind, OSHA will be the driving force for best practice.
Transporting a clean endoscope is a little less black and white. This gray area leaves a small margin for facility interpretation. The crux of the recommendation requires endoscopes must be transported: a) to protect from contamination b) a method to identify endoscope as clean.
The question remains, how? Unfortunately, each facility will need to evaluate their individual environment. There is no clear cut, readily defined method. There are some guiding principles to assist in the development of best practice for your facility. A) Ask the end users for their opinion on how to achieve the goal. They are the experts in flow management 2) Trial the suggestions for several days. What works? What doesn't? 3) Ask your team what barriers are present 4) Ask, if all you could use to communicate are visual environmental cues to identify at what point an endoscope is in the reprocessing process, can you be 100% accurate? If not, go back to the drawing board.
Do you have a burning questions or suggestion which has benefitted your facility? Send an email to [email protected]. Please include your name, facility name and contact information. Perhaps your concern or best practice will be the chosen topic next month. (All personal information will remain anonymous).
|
|
|
Infection Prevention Word Find
|
|
If you are in need of assistance with your infection prevention program, Robin will be able to assist with everything from setting up your program, training your Infection Preventionist, writing or editing Policies & Procedures or just simple telephonic consultation. Robin is taking on-site requests for 2017 at this time. Secure a date on her calendar now.
Please let me know how we can help.
Sincerely,
Cathy Montgomery
Excellentia Advisory Group
[email protected]
636.875.5088 extension 102
See what's happening on our social sites.
|
|
|