|
Join Our List
 |
|
Robin Novak, RN, CIC
|
 |
|
Director of Infection Prevention
and
Endoscopy
636.875.5088 ext. 101
|
|
This Month's Training Opportunities
|
 |
CMS Survey Solutions Session #1
webinar
CMS Survey Solutions #2
CMS Survey
Solutions #3 - Life Safety Code
Over 70 Infection Prevention
topics/presentations available in our library.
|
|
|
|
Volume 1, Number 13
|
November 2017
|
 |
ABOUT ROBIN NOVAK, RN, CIC
Registered Nurse, Certified Infection Preventionist dedicated to disease prevention and high quality healthcare. Strong decision maker who understands the importance of patient, visitor and staff safety following evidence based best practices.
Driven and compassionate healthcare professional with 30 years hands-on experience in fast-paced ambulatory surgery center and hospital environments. Accountable and responsible with an additional focus on Quality Assurance Process Improvement
.
In the past, Robin has served as the SGNA Carolina Chapter President, involved in SGNA Practice Committee as well as a Regional Committee member. Robin has been active with APIC and is a current member of APIC PALMETTO. Robin was prior employed at the Ambulatory Surgery Center of Spartanburg since 2004 and held roles of Endoscopy Nurse, Endoscopy Charge Nurse and most recently the Quality Assurance Process Improvement Coordinator. Robin has worked on several infection prevention projects for Excellentia Advisory Group including a key role as a faculty speaker at our annual Infection Prevention Strategies for ASC's conference in Las Vegas.
Robin is now Excellentia's Director of Infection Prevention & Endoscopy.
|
| Subscriber Question & My Answer |
I recently presented
Beyond the Infection Control Risk Assessment at a state ASCA meeting. There were some great questions which were posed and I thought I would share one of them here.
The Question:
How do you prioritize which risks to work on first?
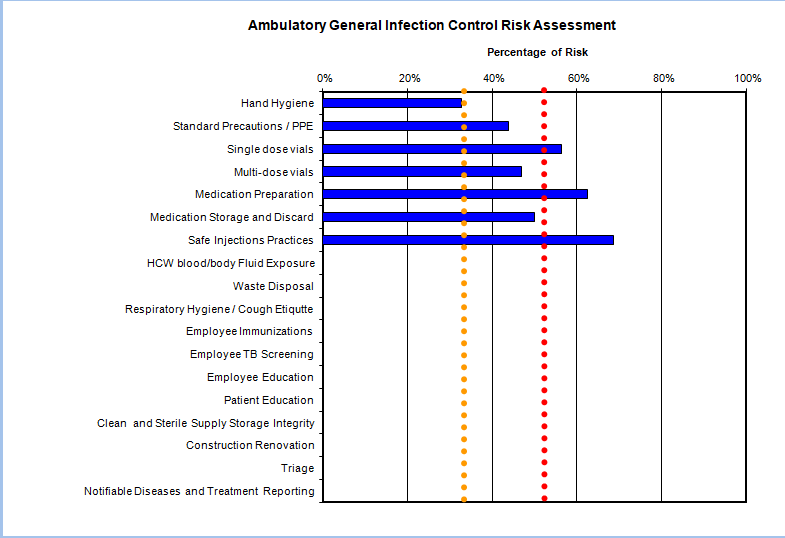
I like to use a risk assessment tool similar to the one many use for the hazard vulnerability assessment. This tool will calculate a percent of risk for you. Now those numbers can be quite intimidating and daunting. It may make you wonder where do I begin this process of correction.
I first meet with my infection control/ QAPI committee. Together we determine what percent would be considered moderate and what would be considered high risk. After setting those thresh holds, then I take the data and put it into a graph. (See below) The graph gives me a quick look and helps me to focus on the outliers.
In the graph
, you can visually see the yellow and red lines which represent the moderate and high thresh holds established by the committee. Those items over the red line are high risk and should be the first priority to address. Those above the yellow line and lower than the red line are moderate risk, They will be the second priority. Now if you have no outliers for the moderate or high thresh hold, then you would choose the top 3-5 highest percentage to begin perfecting.
|
 |
| Critter Craze |
By Robin O. Novak, RN, CIC
Answer to October Critter Craze:
Influenza
Who am I?
-
- Most frequently encountered condition is pharyngitis/ tonsillitis and superficial skin infections
- Sore throat presents with sudden onset of fever, exudative tonsillitis or pharyngitis, tender enlarged anterior cervical lymph nodes.
- Petechiae may be present in background of redness
- Coincident or subsequent otis media may occur
- Rheumatic heart disease may occur days to weeks after acute infection
- Skin infection may proceed through vesicular, pustular and encrusted stages
- Glomerulonephritis may occur later, usually 3 weeks after skin infection
- Necrotizing fascitis is the most severe form of infection from this organism
- A single case is considered an outbreak
- I am gram positive β-hemolytic bacteria
- In the U.S., of the estimated 11,000-13,300 annual severe infections diagnosed, 1,250-1,600 will die
- Incubation period is 1-3 days for pharyngitis and 7-10 days for skin infections
- Transmission: large respiratory droplets OR direct contact with patients or carriers. Rarely with contaminated objects
- Anal, vaginal, skin and pharyngeal carriers have been responsible for nosocomial outbreaks especially following surgical procedures
- Many have been traced to operating room personnel or health care workers
Email Robin at [email protected] with your response. You will receive a personalized reply with validation of the correct answer.
|
| Word on the Street |
- ASC Quality Reporting Specifications Manual-version 7.0 is available and goes into effect 1/1/2018. To learn more, CLICK HERE.
|
|
|
If you are in need of assistance with your infection prevention program, Robin will be able to assist with everything from setting up your program, training your Infection Preventionist, writing or editing Policies & Procedures or just simple telephonic consultation. Robin is taking on-site requests for 2017 at this time. Secure a date on her calendar now.
Please let us know how we can help.
Sincerely,
Cathy Montgomery, RN, CASC Robin Novak, RN, CIC
636-875-5088 extension 102 636-875-5088 ext. 101
See what's happening on our social sites.
|
|
|

