|
|

|
|
Welcome to the June newsletter. The goal of this newsletter is to provide information and analysis of timely topics from recent articles published in the medical literature. I hope you find this information useful and helpful in your health journey.
When I ask my patients to name things that they are worried about as they age, inevitably dementia is one of the top (and often the top) things mentioned. Many of us have grandparents, parents, or other relatives who have suffered with dementia. What can we do now, today, to lower our risk. The first article outlines five lifestyle choices that can lower our risk of dementia by up to 60%. Let's get started!
The second article builds on the first. This time, the focus is just on exercise. How much can regular exercise lower our risk of dementia? What is the mechanism of this improvement? If you are interested in improved executive functioning of your brain check out this article.
Last month we discussed how strenuous exercise didn't harm our knees and may be protective. This month we look at a treatment that can potentially help us when our knees do cause pain. The good news is that this treatment doesn't cause the cartilage degeneration we can see with corticosteroid injections, is inexpensive, and showed no adverse effects.
If you are feeling sick or concerned about symptoms, please call me first. We can discuss your symptoms and decide the best course of action for you, including testing. I now have saliva based COVID-19 tests readily available in my office with 24+ hour turnaround. Serum antibody tests can be performed as well with 24 hour turnaround. Please continue to wash your hands frequently, avoid touching your face, and avoid going out if you are sick.
|
|
Fab Five
|
Five healthy lifestyle choices lower risk for Alzheimer's dementia

How much does our lifestyle matter when it comes to developing dementia? This study reviewed data from two large study populations: the Chicago Health and Aging Project (CHAP), with 1845 participants; and the Memory and Aging Project (MAP), with 920 participants. They defined a healthy lifestyle score on these factors: not smoking; engaging in ≥150 min/wk of physical exercise of moderate to vigorous intensity; light to moderate alcohol consumption; consuming a high-quality Mediterranean-DASH Diet Intervention for Neurodegenerative Delay diet and; engaging in late-life cognitive activities. The overall score ranged from 0 to 5. They followed the groups for a median of 5.8 years in CHAP and 6.0 years in MAP. They found the risk for Alzheimer dementia was 27% lower with each additional lifestyle factor. Compared with participants with zero to one healthy lifestyle factor, those with two to three and four to five healthy lifestyle factors had 37 and 60 percent lower risks for Alzheimer's dementia.
- Objective: To quantify the impact of a healthy lifestyle on the risk of Alzheimer dementia.
- Methods: Using data from the Chicago Health and Aging Project (CHAP; n = 1,845) and the Rush Memory and Aging Project (MAP; n = 920), we defined a healthy lifestyle score on the basis of nonsmoking, ≥150 min/wk moderate/vigorous-intensity physical activity, light to moderate alcohol consumption, high-quality Mediterranean-DASH Diet Intervention for Neurodegenerative Delay diet (upper 40%), and engagement in late-life cognitive activities (upper 40%), giving an overall score ranging from 0 to 5. Cox proportional hazard models were used for each cohort to estimate the hazard ratio (HR) and 95% confidence interval (CI) of the lifestyle score with Alzheimer dementia, and a random-effect meta-analysis was used to pool the results.
- Results: During a median follow-up of 5.8 years in CHAP and 6.0 years in MAP, 379 and 229 participants, respectively, had incident Alzheimer dementia. In multivariable-adjusted models, the pooled HR (95% CI) of Alzheimer dementia across 2 cohorts was 0.73 (95% CI 0.66-0.80) per each additional healthy lifestyle factor. Compared to participants with 0 to 1 healthy lifestyle factor, the risk of Alzheimer dementia was 37% lower (pooled HR 0.63, 95% CI 0.47-0.84) in those with 2 to 3 healthy lifestyle factors and 60% lower (pooled HR 0.40, 95% CI 0.28-0.56) in those with 4 to 5 healthy lifestyle factors.
- Conclusion: A healthy lifestyle as a composite score is associated with a substantially lower risk of Alzheimer's dementia.
In 2018, >50 million people worldwide and 5.7 million Americans were living with Alzheimer's dementia. As the population ages, it is projected that the prevalence of Alzheimer's dementia will triple in the next 30 years so the need for prevention and treatment strategies is large. This study sought to combine several individual factors known to favor improvement or slowing of Alzheimer's onset. As expected, an increased number of healthy lifestyle behaviors was associated with a lower risk of Alzheimer's dementia. Those who had 4-5 healthy behaviors simultaneously had a 60% lower risk of developing dementia than those with 0-1 healthy habits, regardless of genetic predisposition. Take-home points are: don't smoke (quit ASAP if you do); get at least moderate activity daily (20+ minutes); light to moderate alcohol intake (0-1 drinks daily for women and 0-2 for men); eat a diet low in sugar, processed foods, high in fiber, vegetables, fruits, healthy fats; and keep your mind active. I would add appropriate blood pressure control to this formula. This can initiate a chain of metabolic and molecular alterations that inhibit inflammation and oxidative stress and may reduce the amyloid accumulation, neuritic plaques, and neurofibrillary tangles seen in the brains of Alzheimer's dementia patients.
|
|
|
Aerobic exercise improves thinking and cerebrovascular regulation
We assume normal aging involves both physical and cognitive decline. We have increased arterial stiffness due to endothelial dysfunction which limits the ability of the arteries to dilate and results in decreased blood flow and functional decline of memory, processing speed, and executive function. Exercise has been shown to improve memory, attention, executive functioning, and cerebrovascular perfusion. This study followed a group of healthy older adults (average age 65) over 6 months who were enrolled in a supervised exercise program. The researchers found improvements in participants' performance in several cognitive areas, improvement in cardiorespiratory fitness, and resting measures of cerebrovascular function.
Abstract:
- Objective: To test the hypothesis that aerobic exercise is associated with improvements in cognition and cerebrovascular regulation, we enrolled 206 healthy low-active middle-aged and older adults (mean ± SD age 65.9 ± 6.4 years) in a supervised 6-month aerobic exercise intervention and assessed them before and after the intervention.
- Methods: The study is a quasi-experimental single group pre/postintervention study. Neuropsychological tests were used to assess cognition before and after the intervention. Transcranial Doppler ultrasound was used to measure cerebral blood flow velocity. Cerebrovascular regulation was assessed at rest, during euoxic hypercapnia, and in response to submaximal exercise. Multiple linear regression was used to examine the association between changes in cognition and changes in cerebrovascular function.
- Results: The intervention was associated with improvements in some cognitive domains, cardiorespiratory fitness, and cerebrovascular regulation. Changes in executive functions were negatively associated with changes in cerebrovascular resistance index (CVRi) during submaximal exercise (β = −0.205, p = 0.013), while fluency improvements were positively associated with changes in CVRi during hypercapnia (β = 0.106, p = 0.03).
- Conclusion: The 6-month aerobic exercise intervention was associated with improvements in some cognitive domains and cerebrovascular regulation. Secondary analyses showed a novel association between changes in cognition and changes in cerebrovascular regulation during euoxic hypercapnia and in response to submaximal exercise.
Aging is associated with a decreased cerebrovascular reserve which can lead to hypoperfusion and may contribute to an increased risk of ischemic injury and Alzheimer's disease. This study aligns with others showing that increases in fitness result in improved executive functioning and processing speeds. Additionally, improved cerebral blood flow is seen after exercise which has been linked to improved verbal fluency. This builds on the findings from the first study that staying active is very important for brain health.
|
|
Some Sugar For Your Knees
|
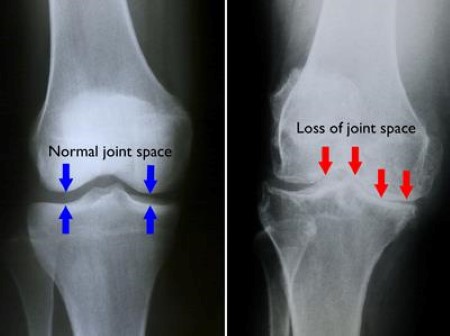
Intra-articular dextrose improves symptoms of knee arthritis
Knee osteoarthritis (OA) is the most common joint disorder in the United States.
Among adults 60 years of age or older the prevalence
of symptomatic knee OA
is approximately 10% in men and 13% in women. One of the common treatments for knee pain from osteoarthritis is a cortisone (steroid) injection, however, effects are short-lasting and studies have shown knee cartilage volume loss with repetitive injections over a 2-year period. Dextrose injections (prolotherapy) has been used for over 60 years and is an inexpensive treatment with an excellent safety profile. Dextrose is a sugar-water solution. The standard prolotherapy injection protocol involves a whole joint approach, with both intra-articular injections into synovial spaces and extra-articular injections at soft tissue bony attachments. The standard procedure is uncomfortable because of the multiple injections required. This study was a 1 year blinded randomized controlled trial to assess the efficacy of intra-articular dextrose prolotherapy. Intra-articular dextrose injections reduced pain and improved function and quality of life compared with normal saline injections and these beneficial effects endured through the 52 weeks of the study. No adverse events were reported.
- PURPOSE: To test the efficacy of intra-articular hypertonic dextrose prolotherapy (DPT) vs normal saline (NS) injection for knee osteoarthritis (KOA).
- METHODS: A single-center, parallel-group, blinded, randomized controlled trial was conducted at a university primary care clinic in Hong Kong. Patients with KOA (n = 76) were randomly allocated (1:1) to DPT or NS groups for injections at weeks 0, 4, 8, and 16. The primary outcome was the Western Ontario McMaster University Osteoarthritis Index (WOMAC; 0-100 points) pain score. The secondary outcomes were the WOMAC composite, function and stiffness scores; objectively assessed physical function test results; visual analogue scale (VAS) for knee pain; and EuroQol-5D score. All outcomes were evaluated at baseline and at 16, 26, and 52 weeks using linear mixed model.
- RESULTS: Randomization produced similar groups. The WOMAC pain score at 52 weeks showed a difference-in-difference estimate of −10.34 (95% CI, −19.20 to −1.49, P = 0.022) points. A similar favorable effect was shown on the difference-in-difference estimate on WOMAC function score of −9.55 (95% CI, −17.72 to −1.39, P = 0.022), WOMAC composite score of −9.65 (95% CI, −17.77 to −1.53, P = 0.020), VAS pain intensity score of −10.98 (95% CI, −21.36 to −0.61, P = 0.038), and EuroQol-5D VAS score of 8.64 (95% CI, 1.36 to 5.92, P = 0.020). No adverse events were reported.
- CONCLUSION: Intra-articular dextrose prolotherapy injections reduced pain, improved function and quality of life in patients with KOA compared with blinded saline injections. The procedure is straightforward and safe; the adherence and satisfaction were high.
Last month we discussed a study showing that
people who engaged in exercise, especially low to moderate exercise did not experience an increase in their risk of developing knee arthritis, and in fact, the exercise may be protective. This month, we look at a possible treatment for people who have arthritis. This study randomized 76 subjects to receive either a saline injection or a dextrose injection. They found statistically significant improvement in the dextrose group as compared to the saline group. There were no adverse effects from the injections. The saline group did show improvement which has been seen in other head to head studies with comparing stem cell injections to saline (no difference by the way). Cortisone injections can provide temporary relief and can be useful for acute flares in the knee. Hyaluronic acid injections have a peak relief at 8 weeks but then effects begin to decrease. Intra-articular dextrose injections reduced pain, improved function, and quality of life compared with saline injections, and these beneficial effects endured through a year. No adverse events were reported and satisfaction with the procedure was high. I have been doing this type of dextrose injection for many years. There have been several studies supporting this practice coming out especially over the past 5-10 years. It is a nice adjunct for people having problems with their knees. I would like to see a study comparing dextrose injection to platelet-rich plasma injection as this has also been giving people relief.
|
|
Thank you for taking the time to read through this newsletter. I hope you have found this information useful as we work together to optimize your health. Feel free to pass this on to anyone you think would benefit from this information.
You can find previous newsletters archived on my website here.
As always, if you have questions about anything in this newsletter or have topics you would like me to address, please feel free to contact me by
email
, phone, or just stop by!
To Your Good Health,
Mark Niedfeldt, M.D.
|
|
|