|
|
MUSC Otolaryngology - Head & Neck Surgery E-Update November 2016
|
|
Colleagues,
Our ENT E-Updates are designed to provide brief, practical, clinical updates in areas where we all struggle in managing our patients. I hope you are finding these newsletters useful. Your feedback or questions about the E-Update articles, your patients, or any other ENT issue are always welcome. Write to us at entupdate@musc.edu - And please forward this E-Update to your colleagues who may also benefit from sharing the latest ENT topics. As always, your support is deeply appreciated.
Yours sincerely,
Paul R. Lambert, M.D.
Professor and Department Chair
|
Oral Cavity and Oropharyngeal Cancer:
A New Staging System for 2017
Masanari G. Kato, B.S., Terry A. Day, M.D.
|
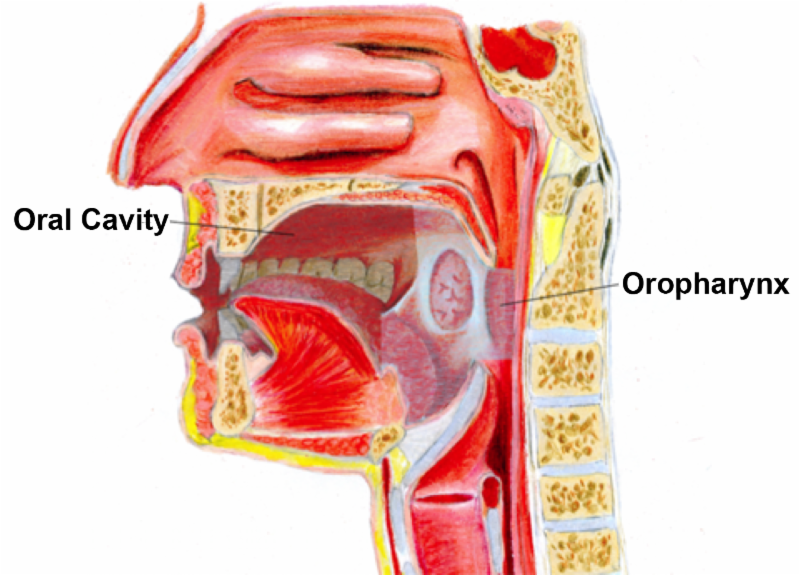
Figure 1. The anatomy of the oral cavity and the oropharynx (used with permission from artist, Lauren Visserman).
|
|
INTRODUCTION
Historically, squamous cell carcinomas of the oral cavity (OCSCC) and oropharynx (OPSCC) have been grouped together as similar diseases with the terms "oral" and "oropharyngeal" used synonymously. The use of these terms interchangeably has since become obsolete, as translational and clinical research has distinguished one from the other in many respects other than just anatomic site, such as by risk factors, patient demographics, etiopathogenesis, and management.
These, among other emerging findings, have resulted in evidence that the 7th ed. (2010) American Joint Committee on Cancer (AJCC) staging system may not accurately reflect the differences in stage-related prognosis as a resource to guide treatment. Recently, the AJCC released the 8th ed. of the cancer staging manual, effective January 1st 2017. With this new staging system, notable modifications taken from the latest published research have occurred and are expected to influence current management guidelines.
|
BACKGROUND
Anatomy
The anatomic separation of the subsites and borders of the oral cavity and oropharynx are often confused, though important to the diagnosis and management of OCSCC and OPSCC. The former begins at the mucocutaneous junction of the lips and extends posteriorly, including the alveolar ridge and gums, the anterior two-thirds of the tongue, floor of the mouth, buccal mucosa, retromolar trigone, and hard palate (
Figure 1).
The oropharynx begins superiorly at the junction of the soft and hard palate, and inferiorly at the circumvallate papilla of the tongue. Subsites of the oropharynx include the soft palate, tonsillar pillars, tonsils, base (posterior 1/3) of the tongue, vallecula, and the pharyngeal walls, and is bounded superiorly by the lower surface of the soft palate and inferiorly by the epiglottis (Figure 1).
1
Epidemiology
Head and neck cancers (HNC) make up 3% of all cancers in the United States, with a favorable, downward trend in its overall occurrence.
2,3
The rate of OCSCC has paralleled this pattern while OPSCC incidence has been accelerating (Figures 2A, 2B).
2
This observation is due to the surge in human papilloma virus (HPV) associated OPSCCs, approaching 60-80% of all OPSCCs, a subset now often referred to as an "epidemic" in the head and neck community.
4,5
Of note, the incidence of "tongue" cancer is inferred to account for both the oral tongue and base of tongue by both the Surveillance, Epidemiology, and End Results (SEER) database and American Cancer Society, and its rise due to increasing rates of the latter, which is a distinct subsite of the oropharynx (Figure 2A). Thus, Figure 2A shows rising "tongue" cancer, which appears to be primarily a result of the increase in base of tongue as can be appreciated in Figure 2B. Researchers are optimistic that future national databases will separate tongue into the "oral" part of the tongue and separate the "base of tongue" into the oropharynx. Between OCSCC and OPSCC, the American Cancer Society estimates nearly 50,000 new cases will develop, leading to almost 10,000 deaths in the US for 2016 alone.
3
|
|
Figure 2.
Age-adjusted SEER incidence rates by subsite in the U.S., all races, both sexes from 1975-2013. A. OCSCC declining overall.2 Of note, the incidence of tongue cancer is inferred to account for the oral tongue and base of tongue, and its rise due to increasing rates of the latter, a distinct subsite of the oropharynx B. Rates of OPSCC rising rapidly.2
|
Patient Demographics and Clinical Characteristics
It is interesting that HPV-positivity in the oropharynx patients represent a unique entity, as the HPV-negative OPSCC and all OCSCC patients appear to be similar in demographics. This distinction along with other clinical characteristics of each is summarized below (
Table 1).
|
Table 1
. Common Demographics and Clinical Characteristics of OCSCC and OPSCC
|
|
The initial workup of these patients involves a physical exam, visualizing the primary tumor by fiberoptic endoscopy in the outpatient clinic, and sampling the primary tumor with a tissue biopsy or neck mass with fine needle aspiration to confirm the disease. Currently, testing for HPV status is routine for oropharyngeal lesions, immunostaining for p16 protein (surrogate marker) being the most popular method. Moreover, when encountering neck masses proven to be squamous cell carcinoma, p16 testing could be utilized to predict HPV and/or oropharyngeal origin. Following diagnosis, imaging modalities such as MRI, CT, and CT-PET are often utilized to determine the extent of disease, namely, nodal involvement and the presence of distant metastasis.
Imaging
Typically, contrasted CT or MRI of the primary lesion and the neck is employed for both OCSCC and OPSCC, with CT-PET reserved for advanced disease. For OPSCC, the authors feel that contrasted CT combined with the CT-PET fusion is a useful and beneficial imaging study that provides information on primary tumor proximity to the lingual neurovascular bundle, the carotid and jugular vascular structures, along with mandible and pterygoid muscles, which aids in accurate staging (Figure 3A). Additionally, contrasted imaging reveals lymph nodes that may be suspicious for harboring metastatic disease even when they are normal by size criteria (Figure 3B). As noted earlier, HPV-positive OPSCC commonly involves the base of tongue (Figure 4A) and advanced nodal disease is more likely present, typically appearing large and cystic (Figure 4B).
|
Figure 3.
Imaging of Advanced OCSCC. A. CT-PET showing uptake of primary gingival SCC involving the mandible (green arrow) with nodal metastasis (yellow arrows) B. Contrast CT showing a lymph node less than 1cm in size (red arrow) with metastatic OCSCC.
|
|
Figure 4.
Imaging of Advanced OPSCC. A. CT-PET showing uptake of primary base of tongue SCC (green arrow) with nodal metastasis (yellow arrow) B. Contrast CT showing a cystic lymph node (red arrows) with metastatic OPSCC.
|
Staging
The clinical assessments outlined above then translate to the clinical stage of the cancer. Like most cancers, OCSCC and OPSCC are staged by the TNM (tumor, node, metastasis) staging system, a classification established by the AJCC to categorize cancer patients based on prognostic differences. The resulting alphanumeric code (T
0-4,
N
0-3
, M
0-1
) then corresponds to an overall stage (I to IV).
|
EMERGING CONCEPTS
Since the implementation of the previous AJCC staging system (7th ed., 2010), treatment standards, patient demographics, and cancer knowledge have evolved. A number of these findings relate to improving the accuracy of the staging system, while others shed light on future strategies to undertake the HPV-positive OPSCC epidemic. Changes in staging have resulted from studies revealing prognostic indicators that impact treatment, locoregional control, and survival.
Oral Cavity Cancer
Findings related to OCSCC vary,8-12 though notably, the depth of invasion (DOI) of the primary tumor was found to be an independent prognostic measure for both nodal metastasis and survival in OCSCC.13-15 The DOI is measured histologically by utilizing the basement membrane of normal adjacent tissue as reference. Incorporating the DOI by increments of 5mms helps to categorize patients by survival more effectively compared to the 7th ed. staging system.13,14
Oropharyngeal Cancer
Evidence supporting changes related to OPSCCs has been far more drastic. The stark contrasts in clinical disease behaviors and prognoses between HPV-positive and HPV-negative OPSCCs have caused the 7th ed. staging to prove ineffective. This is based on the account of the increase in HPV-positive disease, which tends to have smaller primary tumors and more advanced nodal involvements.16 Due to these clinical characteristics, HPV-positive patients are frequently given the diagnosis of advanced stage OPSCC, though outcomes are much more favorable compared to their HPV-negative counterpart.17,18 Evidence now reveals that previous classifications of nodal disease as well as local invasiveness in HPV-positive OPSCC must be reconsolidated to more accurately reflect prognostic differences between disease stages.18 These observations, in addition to numerous others, have led to the proposition for a separate staging system for HPV-related OPSCCs.17-24
Extranodal Extension
The presence of extranodal extension (ENE) is defined as the extension of malignancy through the capsule of an affected lymph node. Depending on its severity, it could be recognized clinically, radiographically, or histologically. It's known to be a poor prognostic marker indicating an increased likelihood of regional recurrence and distant metastasis, and as a result, propositions for its addition to the staging system have been made.25,26 Interestingly, ENE is not as predictive of a negative outcome in HPV-positive OPSCC as it is in HPV-negative OPSCC and other HNSCC sites.27
HPV Vaccination
High-risk HPV serotypes (16 and 18) are well known for causing cancers at various sites, namely the cervix, resulting in the development of a number of effective adolescent-administered vaccines. The question as to whether they translate, if at all, to the prevention of HPV-associated OPSCC is logical, but would be substantially difficult to study. However, there are implications of their benefit, and therefore, adolescents of both genders are recommended vaccination.28
At the same time, other novel vaccines with the potential to prevent and even treat HPV-positive HNC are in the works. Many of these approaches are in their infancy and manipulate HPV's E6 and E7 proteins, the core of the virus' tumorigenic virulence.29,30 Injections containing genetically modified HPV-positive cancer cells and E6 and E7-fused proteins are some future developments that may hold promise.31-34 |
THE NEW STAGING SYSTEM (8th ed.)
A rigorous review of the accumulating data has resulted in the 8th iteration of the AJCC staging system (2017), major modifications for which are outlined below (Table 2)35. It is also imperative to note the separate clinical and pathological TNM stage grouping systems unique to HPV-positive OPSCC. In brief, clinical Stage I category is expanded to include T0-T2 with cN0-N1 disease, while T3 or cN2 disease would upstage to clinical Stage II, and T4 or cN3 disease would upstage to clinical Stage III. Similarly, T0-T2 with pN0-N1 disease is considered pathological Stage I, however, pathological Stage II is rearranged to include T3-T4 with pN0-N1 and T0-T2 with pN2 conditions, and pathological Stage III is limited to T3-T4 with pN2 disease. Of note, clinical and pathological Stage IV disease is only determined by the presence of distant metastasis (M1) and pathological N3 no longer exists.35
|
Table 2.
Summary comparing 7th and 8th ed. AJCC staging of OCSCC and OPSCC
34
DOI - depth of invasion, LN - lymph node, ENE(+) - extranodal extension present, ENE(-) extranodal extension absent, ipsi - ipsilateral, bi - bilateral, ctr - contralateral
|
CHANGES IN MANAGEMENT
Current therapies for OCSCC and OPSCC include isolated or various combinations of surgery, radiation therapy, chemotherapy, and immunotherapy. The management has historically been stage-dependent, with therapies increasing in intensity with higher stage. In general, all OCSCCs are treated with surgery unless metastatic, unresectable, or there are contraindications to surgery. However, OPSCC can be treated with surgery (transoral robotic surgery) or radiation therapy alone for early stage (I or II) while combined therapy using surgery plus radiation therapy or chemoradiation is the standard for advanced stage (III or IV).
36,37
However, recent evidence suggests the need to individually tailor treatment practices as overtreatment has been a topic of concern, particularly for early-stage OCSCCs and OPSCCs.
18,38
Consequently, prospective studies are currently underway to minimize morbidities and de-intensifying treatment in patients undergoing aggressive multimodal regimens.
23
|
SUMMARY
OCSCC and OPSCC are clinically and pathologically distinct diseases. While the overall decrease in incidence of all HNCs is favorable, the rise in HPV-positive OPSCCs has become an important issue in the diagnosis, prevention, and treatment of these cancers. This evolving landscape in the modern era has culminated in the release of the 8th ed. of the AJCC staging system, which incorporates critical parameters to improve prognostic categorization. Highlights include the incorporation of depth of invasion in oral tongue cancers, separation of OPSCC staging by HPV status, and inclusion of extranodal extension in nodal staging. By more accurately reflecting the differences in patient prognoses, cancer management is sure to adapt with time. Furthermore, translational research is showing potential in the realm of HPV prevention, diagnostics, and unique therapeutics, adding to the collective efforts to tackle this epidemic.
|
References
- Murphy B, Day TA. Oral vs. Oropharyngeal Cancer, Compare & Contrast. Available here.
- Park SJ, Yang NR, Seo EK. Vestibular schwannoma atypically invading temporal bone. Journal of Korean Neurosurgical Society 2015; 57:292-294.
- American Cancer Society. Cancer Facts & Figures 2016, 2016.
- Polednak AP. Using Data on Tumor Grade in Cancer Registries to Enhance Surveillance of Oropharyngeal Cancers in Relation to the Human Papillomavirus Epidemic. Journal of registry management 2016; 43:29-35.
- Mehanna H, Beech T, Nicholson T, et al. Prevalence of human papillomavirus in oropharyngeal and nonoropharyngeal head and neck cancer--systematic review and meta-analysis of trends by time and region. Head Neck 2013; 35:747-755.
- Gillison ML, D'Souza G, Westra W, et al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst 2008; 100:407-420.
- McIlwain WR, Sood AJ, Nguyen SA, Day TA. Initial symptoms in patients with HPV-positive and HPV-negative oropharyngeal cancer. JAMA otolaryngology-- head & neck surgery 2014; 140:441-447.
- Patel SG, Amit M, Yen TC, et al. Lymph node density in oral cavity cancer: results of the International Consortium for Outcomes Research. Br J Cancer 2013; 109:2087-2095.
- Ebrahimi A, Gil Z, Amit M, et al. The prognosis of N2b and N2c lymph node disease in oral squamous cell carcinoma is determined by the number of metastatic lymph nodes rather than laterality: evidence to support a revision of the American Joint Committee on Cancer staging system. Cancer 2014; 120:1968-1974.
- Ebrahimi A, Gil Z, Amit M, et al. Comparison of the American Joint Committee on Cancer N1 versus N2a nodal categories for predicting survival and recurrence in patients with oral cancer: Time to acknowledge an arbitrary distinction and modify the system. Head Neck 2016; 38:135-139.
- Boland PW, Pataridis K, Eley KA, Golding SJ, Watt-Smith SR. A detailed anatomical assessment of the lateral tongue extrinsic musculature, and proximity to the tongue mucosal surface. Does this confirm the current TNM T4a muscular subclassification? Surg Radiol Anat 2013; 35:559-564.
- Kuk SK, Yoon HJ, Hong SD, Hong SP, Lee JI. Staging significance of bone invasion in small-sized (4cm or less) oral squamous cell carcinoma as defined by the American Joint Committee on Cancer. Oral Oncol 2016; 55:31-36.
- Ebrahimi A, Gil Z, Amit M, et al. Primary tumor staging for oral cancer and a proposed modification incorporating depth of invasion: an international multicenter retrospective study. JAMA Otolaryngol Head Neck Surg 2014; 140:1138-1148.
- Hubert Low TH, Gao K, Elliott M, Clark JR. Tumor classification for early oral cancer: re-evaluate the current TNM classification. Head Neck 2015; 37:223-228.
- Kane SV, Gupta M, Kakade AC, A DC. Depth of invasion is the most significant histological predictor of subclinical cervical lymph node metastasis in early squamous carcinomas of the oral cavity. Eur J Surg Oncol 2006; 32:795-803.
- Marur S, D'Souza G, Westra WH, Forastiere AA. HPV-associated head and neck cancer: a virus-related cancer epidemic. Lancet Oncol 2010; 11:781-789.
- Huang SH, Xu W, Waldron J, et al. Refining American Joint Committee on Cancer/Union for International Cancer Control TNM stage and prognostic groups for human papillomavirus-related oropharyngeal carcinomas. J Clin Oncol 2015; 33:836-845.
- O'Sullivan B, Huang SH, Su J, et al. Development and validation of a staging system for HPV-related oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICON-S): a multicentre cohort study. Lancet Oncol 2016; 17:440-451.
- Rios Velazquez E, Hoebers F, Aerts HJ, et al. Externally validated HPV-based prognostic nomogram for oropharyngeal carcinoma patients yields more accurate predictions than TNM staging. Radiother Oncol 2014; 113:324-330.
- Beitler JJ, LeCraw Mikell J, Switchenko J. Human Papillomavirus-Related Oropharyngeal Cancer: Agree With a New Staging System, but the Devil Is in the Details. J Clin Oncol 2015; 33:3217-3218.
- Keane FK, Chen YH, Neville BA, et al. Changing prognostic significance of tumor stage and nodal stage in patients with squamous cell carcinoma of the oropharynx in the human papillomavirus era. Cancer 2015; 121:2594-2602.
- Dahlstrom KR, Garden AS, William WN, Jr., Lim MY, Sturgis EM. Proposed Staging System for Patients With HPV-Related Oropharyngeal Cancer Based on Nasopharyngeal Cancer N Categories. J Clin Oncol 2016; 34:1848-1854.
- Horne ZD, Glaser SM, Vargo JA, et al. Confirmation of proposed human papillomavirus risk-adapted staging according to AJCC/UICC TNM criteria for positive oropharyngeal carcinomas. Cancer 2016; 122:2021-2030.
- Keane FK, Chen YH, Tishler RB, et al. Population-based validation of the recursive partitioning analysis-based staging system for oropharyngeal cancer. Head Neck 2016.
- Wreesmann VB, Katabi N, Palmer FL, et al. Influence of extracapsular nodal spread extent on prognosis of oral squamous cell carcinoma. Head Neck 2016; 38 Suppl 1:E1192-1199.
- Wenzel S, Sagowski C, Kehrl W, Metternich FU. The prognostic impact of metastatic pattern of lymph nodes in patients with oral and oropharyngeal squamous cell carcinomas. Eur Arch Otorhinolaryngol 2004; 261:270-275.
- Sinha P, Lewis JS, Jr., Piccirillo JF, Kallogjeri D, Haughey BH. Extracapsular spread and adjuvant therapy in human papillomavirus-related, p16-positive oropharyngeal carcinoma. Cancer 2012; 118:3519-3530.
- Lowy DR, Herrero R, Hildesheim A. Primary endpoints for future prophylactic human papillomavirus vaccine trials: towards infection and immunobridging. Lancet Oncol 2015; 16:e226-233.
- Dyson N, Howley PM, Munger K, Harlow E. The human papilloma virus-16 E7 oncoprotein is able to bind to the retinoblastoma gene product. Science 1989; 243:934-937.
- Scheffner M, Werness BA, Huibregtse JM, Levine AJ, Howley PM. The E6 oncoprotein encoded by human papillomavirus types 16 and 18 promotes the degradation of p53. Cell 1990; 63:1129-1136.
- Mikyskova R, Indrova M, Simova J, Bieblova J, Bubenik J, Reinis M. Genetically modified tumour vaccines producing IL-12 augment chemotherapy of HPV16-associated tumours with gemcitabine. Oncol Rep 2011; 25:1683-1689.
- Mansilla C, Berraondo P, Durantez M, et al. Eradication of large tumors expressing human papillomavirus E7 protein by therapeutic vaccination with E7 fused to the extra domain a from fibronectin. Int J Cancer 2012; 131:641-651.
- Venuti A, Curzio G, Mariani L, Paolini F. Immunotherapy of HPV-associated cancer: DNA/plant-derived vaccines and new orthotopic mouse models. Cancer Immunol Immunother 2015; 64:1329-1338.
- Yin W, Duluc D, Joo H, et al. Therapeutic HPV Cancer Vaccine Targeted to CD40 Elicits Effective CD8+ T-cell Immunity. Cancer Immunol Res 2016; 4:823-834.
- AJCC Cancer Staging Manual. In: Amin MB, Edge S, Greene FL, Byrd DR, Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR, Sullivan DC, Jessup JM, Brierley JD, Gaspar LE, Schilsky RL, Balch CM, Winchester DP, Asare EA, Madera M, Gress DM, Meyer LR, eds.: Springer International Publishing, 2017.
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Head and Neck Cancers. In: Network NCC, ed., 2016.
- Sher DJ, Rusthoven CC, Khan SA, Fidler MJ, Zhu H, Koshy M. National patterns of care and predictors of neoadjuvant and concurrent chemotherapy use with definitive radiotherapy in the treatment of patients with oropharyngeal squamous cell carcinoma. Cancer 2016.
- Cracchiolo JR, Baxi SS, Morris LG, et al. Increase in primary surgical treatment of T1 and T2 oropharyngeal squamous cell carcinoma and rates of adverse pathologic features: National Cancer Data Base. Cancer 2016; 122:1523-1532.
|
|
Terry A, Day, M.D.
Wendy and Keith Wellin Endowed Chair in Head & Neck Surgery
Professor and Director,
Division of Head & Neck Oncology
M.D.: University of Oklahoma College of Medicine
Residency: Louisiana State University Medical Center
Fellowship: University of California, Davis, for Head & Neck Oncologic Surgery
University of Bern in Switzerland for Craniomaxillofacial Surgery
Special Interests: Head & Neck tumor surgery, microvascular reconstructive surgery, skull base surgery
Email: dayt@musc.edu
|
|
E-Update Articles
Look for these articles in upcoming issues
December:
Status of Sustained Release Dexamethasone in Treating Meniere's Disease
January:
Caustic Ingestion in Children
February:
Facial Plastic & Reconstructive Surgery
To view any of our past E-Updates visit our
|
|
Continuing Education
November 11, 2016
__________________
|
|
|
|
|
|
|