|
|
MUSC Otolaryngology - Head & Neck Surgery E-Update April 2016
|
|
Greetings Colleagues!
Our ENT E-Updates are designed to provide brief, practical, clinical updates in areas where we all struggle in managing our patients. I hope you are finding these newsletters useful. Your feedback or questions about the E-Update articles, your patients, or any other ENT issue are always welcome. Write to us at entupdate@musc.edu - And please forward this E-Update to your colleagues who may also benefit from sharing the latest ENT topics. As always, your support is deeply appreciated.
Yours sincerely,
Paul R. Lambert, M.D.
Professor and Department Chair
|
|
Head & Neck Staging Changes Coming in the
8th AJCC Cancer Staging Manual
Joshua D. Hornig, M.D., FRCS(C)
|
Assigning patients the proper clinical and pathological stage is one of the most important aspects of clinicians who are involved with patients with cancer. Recently, there has been a recognition of new pathological features of primary tumors and cervical lymph node metastasis that have a strong effect on prognosis.
When using a staging system we want to aim for four tenets: 1) similar survival rates for people put in each stage, 2) each stage should have a different survival than the one above and below it, 3) equal numbers of people in each stage, and 4) the assigned stage should have good approximation of survival for the individual patient. Recently with the onset of HPV related oropharyngeal tumors the 7
th edition survival curves were not as accurate and were failing to uphold the four tenets outlined above. Additionally, new information has come to light that is highlighting the importance of extra nodal extension of disease as well as the importance of depth of invasion of oral cavity cancers. The newest staging system tries to balance the significance of these pathological findings with the existing staging system and aims to have a simpler staging system to increase compliance and reporting.
Changes to the Oropharyngeal Staging
The incidence of oropharyngeal SCCA associated with HPV has been rising at a rate of 5% a year since the early 1990s. Patients who have HPV associated oropharyngeal carcinomas (OPC) are demographically different than non-HPV associated OPC. They are generally younger, healthier with little to no tobacco exposure. HPV OPC is also highly responsive to all forms of treatment and behaves very differently than non-HPV OPC. As the number of HPV OPC rose proportionately, the 7
th staging edition lost the ability to differentiate survival rates between stages and the numerical balance became skewed toward Stage III and Stage IV. So really we are dealing with two separate disease entities that lie in the same anatomical region. As such it was decided to have two separate staging systems for oropharyngeal carcinoma, one for HPV OPC and one for non-HPV OPC.
|
|
Table 1: Clinical and Pathological T category for HPV associated OPC
|
For T stage for HPV associated OPC (
Table 1), T0 has no primary identified, T1 is a tumor <2 cm T2 is <2 cm but less than 4 cm, T3 is larger than 4 cm or extends to the lingual surface of the epiglottis, and T4 is moderately advanced local disease (tumor invades the larynx, extrinsic tongue musculature, medial pterygoid, hard palate, mandible or beyond.
|
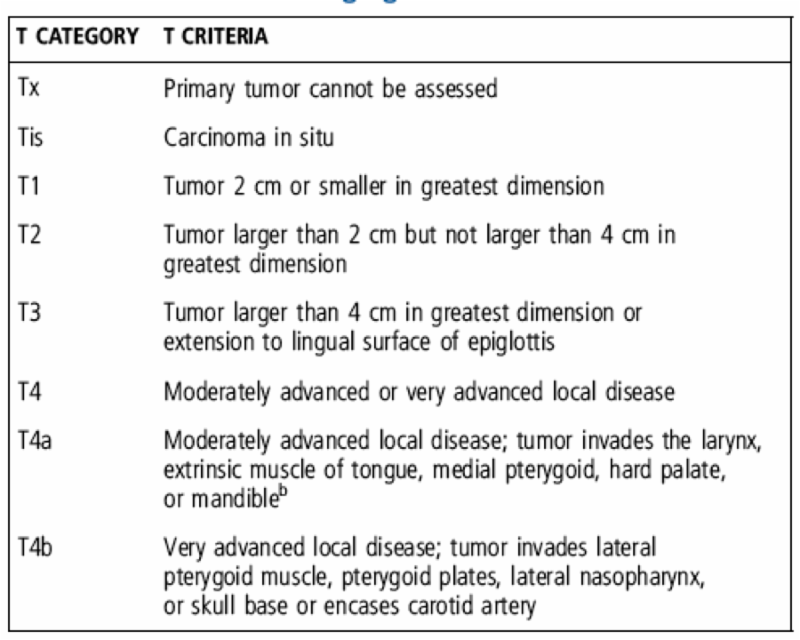
Table 2: Clinical and Pathological T Stage for Non-HPV oropharyngeal carcinoma
Table 3: Clinical N category HPV OPC
|
For non-HPV associated OPC, the T stage system is similar to the 7
th edition. The T stages are as follows (
Table 2): Tx tumors that cannot be assessed, Tis carcinoma in situ, T1 tumor less than 2cm, T2 tumor larger than 2 cm but less than 4 cm, T3 tumor is larger than 4 cm or extends to the lingual surface of the epiglottis and T4a is moderately advanced disease (tumor invades the larynx, extrinsic muscles of the tongue, medial pterygoid, hard palate, or mandible).
Interestingly, nodal disease had a very different impact on survival depending on whether we were talking about HPV OPC or non-HPV OPC. As such a new nodal staging system for HPV OPC was created using clinical criteria (
Table 3) and also for pathologically criteria (
Table 5). The N stage for H, PC OPC is now: Nx nodes cannot be assessed, N0 no regional lymph node mets, N1 one or more ipsilateral lymph nodes (none larger than 6 cm), N2 contralateral or bilateral lymph nodes (none larger than 6 cm), N3 lymph node(s) greater than 6 cm. Even more interesting, and further complicating the staging system in HPV OPC it was found that if you looked at the patients who had a neck dissection and then you looked grouped patients with similar survival data, a new set of pathologically derived N staging was needed. In this scenario, there were only three different N groupings (
Table 5): N0, N1: which is defined as 4 or fewer lymph nodes (size is no longer included) and N2: define as greater than four lymph nodes. This greatly simplifies the pathological N staging and again places this groups into prognostic categories that are significantly different from the other. Please note that only patients who have surgery can be placed into this category.
Additionally, it has become prognostically significant to include extranodal extension (ENE) into the staging system for non-HPV OPC. The new N staging for non-HPV OPC is as follows (
Table 4): Nx regional nodes cannot be assessed, N0 No reginal lymph node mets, N1 are mets in a single ipsilateral lymph node (<3 cm and ENE negative), N2a mets in a single ipsilateral lymph node >3 cm but <6 cm and ENE-negative, N2b mets in multiple ipsilateral lymph nodes all <6 cm and ENE-negative, N2c are bilateral mets or contralateral lymph nodes all <6 cm and ENE-negative, N3a are mets in a lymph node that is larger than 6 cm and ENE-negative, and N3b are mets in any node with clinically overt ENE-positive. So as one can deduce, the presence of ENE is a very poor prognostic variable.
|
Table 4: Clinical N category for non-HPV OPC

|
|
Table 5: Pathologic N Category for HPV OPC

|
|
Finally, to get to an overall stage you need to assess the overall TNM stage. Additionally, because of the incorporation of pathological criteria into HPV OPC, there is now both a clinical HPV OPC stage (
Table 7) and a pathological HPV OPC stage (table 6). There is only one staging system for non-HPV OPC (
Table 8).
|
|
Table 6: Staging System for HPV positive OPC using Pathological Criteria Table
|
Table 7: Clinical Staging System for HPV OPC

|
|
Table 8: Clinical and Pathological Staging System for non-HPV OPC

|
|
|
Joshua D. Hornig, M.D., FRCS(C)
Associate Professor
Head & Neck Oncology
Director, Microvascular Surgery & Functional Outcomes
M.D.: University of Alberta Faculty of Medicine & Dentistry
Residency: University of Alberta
Fellowship: Medical University of South Carolina
Special Interests: Endoscopic thyroid and parathyroid surgery, microvascular reconstruction, head and neck tumors and functional outcomes
Email: hornigjd@musc.edu
|
|
E-Update Articles
Look for these articles in upcoming issues
May:
Resident Education in Otolaryngology
June:
Rhinology
July:
Salivary Endoscopy: A Minimally Invasive Approach to Salivary Gland Disease
To view any of our past E-Updates visit our
|
|
|
|
|
|
|
|
|