News You Need to Know Regulatory News and Updates
|
|
|
TOYON UNIVERSITY® PRESENTS
|
|
INPATIENT PROSPECTIVE PAYMENT SYSTEM PROPOSED RULE - FFY2022
Toyon Associates invites you to a complimentary
one-hour webinar 10:00 a.m. PDT on May 21.
Toyon Associates invites you and your team to a live conversation on the FFY2022 IPPS Proposed Rule. Our discussion will dive into the components of proposed FFY2022 IPPS rates, highlighting areas of significance for providers. Please join us for this important conversation.
This is an important session you won't want to miss.
Register for the webinar HERE.
See you there!
Toyon University® is a virtual 'university' created for our clients. For further information on our curriculum, contact Tim Vanderford at [email protected] or 888.514.9312.
|
|
Inpatient Prospective Payment System Proposed Rule – FFY2022
|
|
|
CMS-1752-P drafted on 4/27/2021; Published in the Federal Register on 5/10/2021 |
On April 27, 2021, the Centers for Medicare & Medicaid Services (CMS) issued the Federal Fiscal Year (FFY) 2022 Inpatient Prospective Payment System (IPPS) Proposed Rule. The Proposed Rule builds on key priorities to close health care equity gaps and support greater access to life-saving diagnostics and therapies during the public health emergency (PHE) and beyond. CMS proposes to create polices supporting a hospital’s readiness to respond to future public health threats and develop the health care workforce in rural and underserved communities. CMS proposes to revise their reporting requirements for scoring, payment, and public quality data in their effort to reduce the adverse impacts of the pandemic and any future unplanned events. The Proposed Rule updates Medicare payment policies and rates for hospitals under the Inpatient Prospective Payment System (IPPS) and the Long-Term Care Hospital (LTCH) Prospective Payment System (PPS), effective for discharges on or after October 1, 2021
Due to the PHE, CMS provides two data sets on the FFY2022 IPPS Proposed Rule Home Page for projecting Medicare IPPS payments in FFY2022. CMS provides data 1) excluding (and before) the PHE; and 2) including the PHE (i.e., “alternative” data). Notably, the alternative data uses discharges and case-mix indices (during the PHE) from FFY2020 MedPAR and FFY2019 cost reports. The proposed data (before the PHE) uses discharges and case-mix indices from FFY2019 MedPAR and FFY2020 cost reports. CMS proposes to use data before the PHE, stating alternative data (inclusive of PHE) is “less suitable for FFY2022 rate setting.” Toyon estimates national FFY2022 IPPS payments excluding PHE data at $130bn, $13bn (11%) greater than estimated national payments of $117bn including PHE data. Please contact Fred Fisher at [email protected] for a free evaluation of CMS’s proposed FFY2022 IPPS payments for your hospital(s).
CMS proposes to establish new requirements and revise existing requirements for the Hospital Value-Based Purchasing (VBP) Program, Hospital Readmissions Reduction Program, Hospital-Acquired Condition (HAC) Reduction Program, Hospital Inpatient Quality (IQR) Reporting Program, Long Term Care Hospital (LTCH) Quality Reporting Program, PPS-Exempt Cancer Hospital Reporting (PCHQR) Program, and the Medicare Promoting Interoperability Program. CMS proposes to “suppress” measurements impacted by the PHE, to “ensure these programs do not reward or penalize hospitals based on circumstances caused by the PHE for COVID-19 that the measures were not designed to accommodate.” In addition, CMS is requesting comments regarding the modernization of the quality measurement enterprise to digital quality measurement.
Overall, the proposed rule is projected to result in an estimated increase of $2.5bn in payments to providers. Included in that amount is a reduction of approximately $0.9bn in Medicare DSH and Uncompensated Care payments. Increases to hospital payments before the DSH and UC reduction for FFY 2022 is $3.4bn (2.8 percent).
Comments must be sent to CMS no later than 5 p.m. EDT on June 28, 2021 at the applicable address provided in each section of the Proposed Rule or submitted electronically at http://www.regulations.gov. When commenting, please refer to file code CMS-1752-P.
Rural Redesignation Update
|
|
|
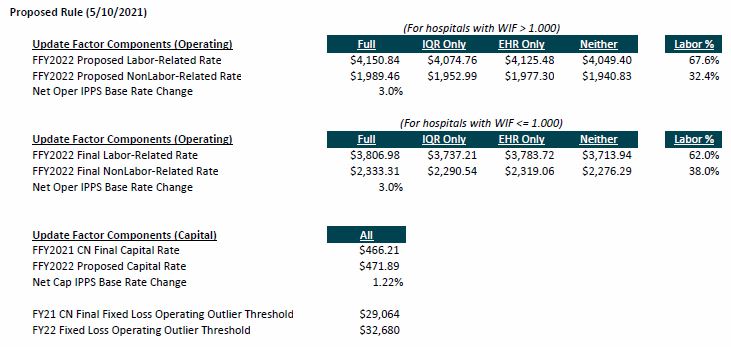
CMS is proposing a base rate increase of 2.8% for hospitals, mostly driven by a market basket increase of 2.5%, reduced by 0.2% and the reversal of the MACRA coding adjustment of 0.5%. A new budget-neutrality factor adjustment was introduced this year to account for the change in Allogeneic Stem Cell Acquisition reimbursement to cost-based. |
|
|
Click here for the full base rate calculation table and comparison to prior year.
|
|
|
Proposed Repeal of Market-based Data Collection, MS-DRG Relative Weights |
CMS proposes to repeal the requirement that a hospital include on the Medicare cost report the median payer-negotiated inpatient services charges for Medicare Advantage organizations by MS-DRG, for cost reporting periods ending on or after Jan. 1.
CMS is also proposing to repeal, effective FFY2024, the market-based MS-DRG relative weight methodology effective that would have used these data to set relative Medicare payment rates for hospital procedures. Rather, CMS would continue using the existing rate-setting methodology for FFY2024 and subsequent years.
|
|
|
Changes to the New COVID-19 Treatments Add-on Payment (NCTAP) |
CMS, in their response to the pandemic established the New COVID-19 Treatments Add-on Payment (NCTAP) for eligible discharges during the Public Health Emergency (PHE). CMS expects that hospitals will continue to witness inpatient cases of COVID-19 beyond the end of the PHE. As a result of CMS’s effort to continue to mitigate potential financial disincentives for hospitals in their providing of new COVID-19 treatments as well as to minimize any potential payment disruption immediately following the end of the PHE, CMS proposes to extend the NCTAP payments for eligible COVID-19 products for through the end of the fiscal year in which the PHE ends.
CMS is also proposing to discontinue NCTAP for discharges on or after Oct. 1, 2021 for a product that is approved for new-technology add-on payments beginning in FFY2022.
|
|
|
Based on the CMS proposed rates for FFY2022, the occupational mix adjusted national average hourly wage is estimated to be $46.37, representing an increase of 2.52% from the prior year.
Continuation of Prior Year Wage Index Policy Changes
CMS proposed and finalized a policy in FFY2020 to reduce wage index high-to-low disparities by increasing the values for low wage index hospitals below the 25th percentile (or a WIF of 0.8418 in FFY2021). In FFY2020, CMS anticipated that it would continue this policy for at least four years, acknowledging that providers in these lower-quartile states would improve employee compensation within four years because of the higher wage index. Accordingly, CMS is proposing to continue this policy in FFY2022. Consistent with the finalized policy in FFY2020 and 2021, in FFY2022 CMS will “fund” this policy by applying a uniform budget neutrality adjustment. The proposed low wage index hospital policy budget neutrality factor is 0.998108 (compared to 0.997970 in FFY2021).
Also, in FFY2020, CMS proposed and finalized a change to the rural floor calculation by removing urban-to-rural reclassifications from the statewide rural floor. CMS is proposing to continue this policy in FFY2022 (as it did in FFY2021) so that state rural floors would be calculated without including the wage data of urban hospitals that have reclassified as rural.
Lastly, in FFY2021, CMS proposed and finalized changes to specific Core-Based Statistical Areas (CBSAs) based on updated census data as released by the Office of Management and Budget (OMB) in its OMB Bulletin No.18-04 dated September 14, 2018. In unprecedented fashion, CMS incorporated the revised OMB delineations to CBSAs impacted in FFY2021, which included new CBSAs, urban counties that became rural counties, rural counties that became urban counties, and existing CBSAs that were split apart. CMS is proposing in FFY2022 to continue to use the OMB delineations adopted beginning with FFY2015 and updated most recently in OMB Bulletin No. 18-04.
As a result of the policy changes noted above, in FFY2020 and FFY2021 CMS finalized a “transition” policy which included a cap of 5% on the decrease of any hospital’s wage index from the prior year. For instance, in FFY2021, a hospital could not receive a final wage index that was less than 5% of what it received in FFY2020. While this transition policy was set to expire in FFY2021 and as proposed, CMS did NOT include a transition policy in FFY2022, CMS acknowledged the ongoing Public Health Emergency (PHE) in the Proposed Rule and is seeking comment on whether it is appropriate to apply a transition policy to the FFY2022 wage index. If CMS were to apply a transition to the FFY2022 wage index for hospitals that are negatively impacted by any of the policy changes described above, CMS is also seeking comment if it is appropriate to apply a transition policy in a budget neutral manner as it did in FFY2020 and FFY2021. In FFY2021, the transition policy’s budget neutrality factor was 0.998851.
Toyon’s Take
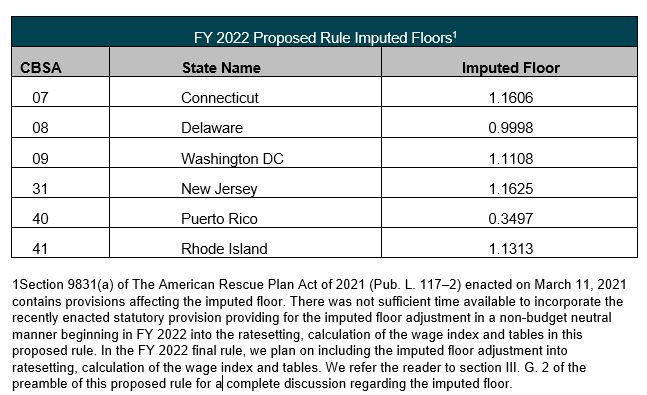
The continuation of the policy changes implemented by CMS over the course of the last two years of rulemaking is not surprising and was anticipated. However, the potential continuation of a transition policy is a bit surprising. The revised OMB delineations notably impacted urban hospitals in the Northeast, primarily New York-New Jersey, as a number of counties were redefined to new CBSA designations and “moved out” of New York City which historically has produced a higher wage index for such hospitals. While the impact to these hospitals was mitigated in FFY2021 due to the transition policy, beyond FFY2021 the impact was likely to be significant and the continuation of a transition policy would be a welcome relief to continue to mitigate this potential impact. However, as noted and discussed further below, a potential transition policy will not mitigate the impact for these hospitals in FFY2022 due to the proposed inclusion of an imputed rural floor for “all-urban” States, which as proposed, includes New Jersey, Delaware, Rhode Island, Washington D.C., and Connecticut.
Toyon applauds CMS's efforts to recognize the PHE and its overall financial impact on the provider community. We encourage hospitals to comment on the proposed transition policy and its potential financial benefit, where applicable, noting that an applied budget neutrality factor of 0.998851 (from FFY2021) will reduce payments overall by approximately 0.10%.
Proposed Occupational Mix Adjustment using Calendar Year (CY) 2019 Survey Data
CMS provides for the collection of data every three years on the occupational mix of employees for each short-term, acute care hospital. In 2016, CMS collected survey data to compute an occupational mix adjustment for the FFY2019, FFY2020 and FFY2021 wage indices. For FFY2022, an updated measurement of occupational mix was required using data from CY2019. CMS is proposing to utilize this data using the same methodology as prior years to calculate an occupational mix adjustment factor. CMS provides analysis in the Proposed Rule pertaining to the impact of the occupational mix adjustment on provider types (e.g., urban vs. rural) which is consistent with previous years. The unadjusted national average hourly wage is $46.42 compared to the occupational mix adjusted national average hourly wage of $46.37.
Reincarnation of the Imputed Rural Floor in “All-Urban” States
In FFY2005, CMS adopted an imputed rural floor policy as a temporary three-year regulatory measure to address concerns from hospitals in all-urban States that argued they were disadvantaged by the absence of rural hospitals to set a wage index floor for those States. After extending the imputed rural floor policy eight times since FFY2005, the policy expired and was not renewed in FFY2018 and has not been included in FFYs 2019 through 2021.
However, as required by Section 9831 of the American Rescue Plan of 2021 enacted on March 11, 2021, CMS proposes to permanently reinstate the imputed rural floor wage index calculation for hospitals located in all-urban States, which refers to States without designated rural areas. In accordance with the American Rescue Plan of 2021, “For discharges occurring on or after October 1, 2021, the area wage index applicable under this subparagraph to any hospital in an all-urban State…may not be less than the minimum area wage index for the fiscal year for hospitals in that State.”
CMS is required by the statute to reinstate the previous imputed rural floor methodology, and this rate cannot be less than the imputed rural floor CMS calculated for such States in FFY2018. Unlike FFY2018 and prior, the new statute specifies that the adjustment pertaining to the imputed rural floor policy shall not be applied in a budget neutral manner, which means that any increase to the wage index for these all-urban States will not be offset by a decrease to the standardized amount or applied to wage indices. Toyon is collaborating with hospitals and associations in these all-urban States to calculate estimate benefit.
In the FFY2022 Proposed Rule, CMS does not account for application of the imputed rural floor impact as there was “not sufficient time available to incorporate the recently enacted statutory provision providing for the imputed floor adjustment in a non-budget neutral manner beginning in FFY2022 into the rate setting, calculation of the wage index and tables…” CMS plans to include the imputed rural floor adjustment into rate setting, calculation of the wage index and tables of the Final Rule.
|
|
|
Other Proposed Changes Impacting Wage Index
- CMS proposes to make two changes to the timing of a hospital’s request to cancel a previously granted reclassification from urban to rural, which would in effect lock a hospital into its rural status for a longer period. CMS acknowledges that these changes are necessary to address the practice of applying for and canceling rural reclassification to influence a State’s rural wage index, which is “detrimental to the stability and accuracy of the Medicare wage index system”. These two changes are described below.
- First, CMS proposes that requests to cancel rural reclassifications be submitted to the CMS Regional Office no earlier than one calendar day after the date when the reclassification became effective, and
- Secondly, CMS proposes to replace an existing rule, which requires cancellation of reclassification no later than 120 days prior to the end of Federal Fiscal Year to be effective at the beginning of the next Federal Fiscal Year, with a requirement that cancellation requests become effective in the Federal Fiscal Year that begins in the Calendar Year after the Calendar Year in which the request was submitted.
- In a separate interim final rule released in conjunction with the Proposed Rule, CMS is applying a decision from 2020 in the U.S. District Court for D.C. that requires CMS to treat hospitals reclassified as rural as rural for the purpose of comparing its average hourly wage data. Previous policy stated that a hospital that opted to reclassify from urban to rural was required to compare its average hourly wage data to that of the urban area where the hospital was physically located rather than the Statewide rural area (e.g., the “106% average hourly wage test”). The court decision ruled that CMS’s previous policy violated the Medicare Act and thereby, CMS is changing its policy effective immediately without a comment period.
- With the release of the FFY2022 Proposed Rule on April 27, 2021, the specified “lock-in” date for hospitals to be included in the rural wage index calculation for FFY2022 is established as proposed as June 28, 2021. In addition, Medicare Geographic Classification Review Board (MGCRB) reclassification withdrawals will need to be submitted to the MGCRB no later than 45 days after the Proposed Rule is published in the Federal Register, which was May 10, 2021, thereby confirming a deadline of June 24, 2021.
Toyon’s Reminder
Reclassified hospitals are not eligible to receive an out-migration factor adjustment, so hospitals that are expected to receive a rural floor wage index (imputed or Statewide rural floor) should consider reclassification withdrawal to secure an outmigration adjustment.
- For all IPPS hospitals whose wage indexes are greater than 1.000, CMS proposes in FFY2022 to apply the wage index to the proposed labor-related share of 67.6% of the national standardized amount, compared to 68.3% in FFY2021.
For additional information regarding wage index changes or updates, please contact Ryan Sader at [email protected]
|
|
|
Proposed Changes to Indirect and Direct Graduate Medical Education (IME and GME) |
There are three provisions contained in the Consolidated Appropriations Act of 2021 (“CAA”) which will affect IME and GME payments to teaching hospitals as well as new requirements for submission of resident data through the Intern and Resident Information System (IRIS).
Additional IME and GME Slots
Section 126 of the CAA will make available 1,000 new resident FTE cap slots funded by Medicare over five years (no more than 200 per year), starting 7/1/2023. These cap slots will be distributed to hospitals that are included in the following four categories:
- Hospitals located in rural areas or that are treated as being in a rural area.
- Hospitals that are training residents over their cap amount
- Hospitals located in the 35 states (listed in the rule) with new medical schools or additional locations and branches of existing campuses.
- Hospitals whose campuses or provider-based facilities serve areas that are designated as Health Professional Shortage Areas (“HPSAs”).
HPSA scores will be a key criterion for all four categories, not just category 4. As an alternative methodology, CMS is considering a prioritization approach for FY 2023 in which the 200 additional residency positions would simply go to hospitals that qualify under one or more of the listed categories. Higher priority is given to those that qualify in multiple categories. Under either methodology, CMS is proposing to limit the new cap slots to 1 FTE per hospital. Applications for the first year’s 200 slots will be due 1/31/2022 for slots effective 7/1/2023.
Proposal for Implementation of Section 127 of the CAA, ‘‘Promoting Rural Hospital GME Funding Opportunity’’
Section 127 of the CAA is intended to provide flexibility for both rural and urban hospitals in partnerships that will focus on the need for additional physicians in rural markets. The agency proposes four changes to the rural training track (“RTT”) program.
-
The first change is in reference to Cap Adjustments for Urban and Rural Hospitals Participating in Rural Training Track Programs. It is proposed that each time a RTT program begins between an urban and rural hospital, both may receive a “rural track FTE limitation” regardless of whether the RTT program meets the newness criteria for Medicare payment purposes.
-
The second change, Cap Adjustments When the Urban Hospital Adds Additional Rural Training Tracks, proposes that urban hospitals with existing RTT caps can receive RTT cap adjustments for additional RTT programs. Rural hospitals would also receive an RTT cap increase.
-
The third proposed change, Removal of Requirement That Rural Track Must Be ‘‘Separately Accredited,’’ would remove the requirement that RTT programs be separately accredited. This is provided that the program in its entirety is accredited by the ACGME, and at least 50% of the residents’ time is spent in rural areas. If these conditions are met, then it may qualify as a RTT and both hospitals (urban and rural) will receive RTT caps.
-
The fourth change, Exemption From the 3-Year Rolling Average During the 5-Year Rural Track FTE Limitation Window, proposes that the RTT program residents will not be included in the hospital’s 3-year rolling average resident cap calculation during the build-up period.
Hospitals Qualifying to Reset Their FTE Resident Caps
Section 131 of the CAA provides an opportunity for hospitals with previously established low or zero per resident amounts and/or FTE caps to establish new per resident amounts (PRA) and FTE caps. Eligible hospitals fall into two categories:
- Category A – hospitals whose PRA and/or resident cap was set based on less than 1.0 FTE in a cost reporting period beginning before October 1, 1997.
- Category B – hospitals whose PRA and/or resident cap was established based on training less than 3.0 FTEs in a cost reporting period beginning on or after October 1, 1997 and before December 27, 2020.
CMS proposes that these eligible Category A hospitals will have a new PRA established if they train at least 1.0 FTE and Category B hospitals would be eligible if they train more than 3.0 FTEs in a cost reporting period beginning on or after December 27, 2020 and before December 26, 2025. In order to be eligible for a revised FTE cap (not for a PRA), the hospital would have to start a brand-new program after 12/27/2020.
Proposal for Intern and Resident Information System (IRIS) Data
Effective for cost reporting periods that begin after October 1, 2021, the regulations (42 C.F.R. § 413.24(f)(5)(i)) that govern IRIS data are proposed to be amended. The amendment will now state that submitted IRIS data must contain the same total counts of direct GME FTE residents (unweighted and weighted) and of IME FTE residents as the total counts of direct GME FTE and IME FTE residents reported in the hospital’s cost report, or the cost report will be rejected for lack of supporting documentation.
Toyon’s Take
The benefit of the additional 1,000 cap slots is quite limited (1 FTE per hospital for each of the five years in the roll-out). Hospitals must commit to increasing their FTE count for the new cap slot(s); they cannot just use them for an existing FTE excess over cap. There will likely be a lot of competition for the 1,000 new cap slots, and CMS is clearly prioritizing hospitals in the most severe HPSAs, using the 1-25 HPSA scale. Other hospitals may not have much of a chance to win the cap slots. While 1,000 new slots is a start, much more relief is needed to have a real impact on national physician shortages.
The RTT rules provide much more flexibility and benefits to hospitals that create these training tracks, by incenting both the urban hospital and its rural partners, and by eliminating some of the prior limitations. The opportunity to re-set PRAs and caps is designed to provide significant relief to the fairly small number of hospitals that were saddled with small PRAs or caps due to the strict application of prior rules.
|
|
|
Implications of Using FFY2019 Data for New Technology Add-on Payment |
IPPS payments are generally based on the most recently available Medicare claims and cost report data. These sources tend to have a lag of 2-to-3 years, and as a result, the statute provides temporary additional payments for cases with high costs under the New Technology Add-on Payment (NTAP) policy.
Medicare, because of this policy, is required to pay the applicable MS-DRG payment rate and up to an additional 65 percent (75 percent for certain antimicrobials) of the cost approved new technology. The new technology add-on payment is not budget neutral and is generally limited to the 2-to 3-year period following the date of the FDA approval or clearance for marketing.
For FFY2022, in connection with CMS’s proposal to use FFY2019 instead of FFY2020 data for FFY2022 IPPS rate setting, CMS is proposing a one-year extension of new technology add-on payments for 14 technologies for which the new technology add-on payment would otherwise be discontinued beginning FFY2022.
|
|
|
Organ Acquisition Payment Policies |
There are several changes CMS proposes regarding the regulation of organ acquisition reimbursement. Some of these changes codify existing Medicare organ acquisition payment policies, that are currently in the Provider Reimbursement Manual (PRM). Other proposed changes codify new organ acquisition payment policies. Please note these changes are CMS’s response to statutory directives in both the recent 21st Century Cures Act, which expanded Medicare coverage for kidney acquisition costs, as well as the Medicare Modernization Act of 2003.
Use of consistent terminology and Proposed definitions
According to CMS, to ensure consistent terminology, CMS proposes to add definitions to 42 C.F.R. § 413.400. This will further define the terms organ, Organ Procurement Organization (OPO), Hospital-Based Organ Procurement Organization (HOPO), transplant hospital (TH), and transplant program (42 C.F.R. 482.70 § 413.400 new subpart L). CMS also will revise the term freestanding (42 C.F.R. § 413.200(b)), histocompatibility laboratory (42 C.F.R. § 493.1227 and 42 C.F.R. § 413.400, new subpart L), and standard acquisition charge. CMS states clarification of these terms and even the proposed definition for organ that differs from the OPO Conditions for Coverage (CfCs), will “mitigate potential stakeholder confusion.”
Organ Acquisition Costs
CMS is proposing to add § 413.402(a) to new subpart L that will codify the 12 elements regarding costs incurred in the acquisition of organs (living/cadaveric by hospital or an OPO). This revision applies existing elements of kidney acquisition costs to all organs and includes additional changes applying to kidney acquisition only (costs for registration of a beneficiary for a kidney transplant and costs for registration of a beneficiary for a non-renal transplant). CMS will also clarify and codify provisions regarding the Standard Acquisition Charges (SACs) for THs/HOPOs. CMS further proposes in this section to limit registration fees to OPTN registration fees based on reasonable cost principles and to codify surgeon fees are “included as kidney acquisition costs only when the kidney excision occurs with a cadaveric donor.”. When a living donor enters the hospital for the actual kidney excision, surgeon fees for excising the kidney are not included as kidney acquisition costs.
Services Not Considered Organ Acquisition Costs
CMS is proposing to establish rules identifying costs that are non-reimbursable which may be incurred during organ acquisition and transplant, including, but not limited to: burial and funeral expenses for cadaveric donors, costs associated with transportation of a living or cadaveric donor, costs incurred prior to a potential donor being declared brain dead, fees or in-center payments for donor referrals, costs associated with OPO sponsored seminars where continuing education credits are given, and certain costs incurred for administrator’s duties associated with professional organizations.
Medicare’s Share of Acquisition Costs and Counting of Organs
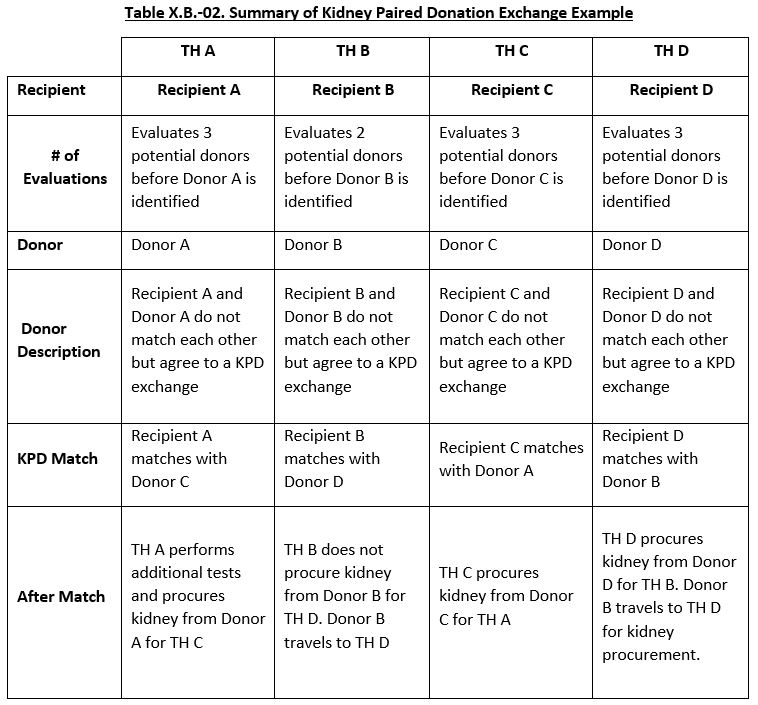
CMS is proposing to change their policy in the identification of each donor beneficiary to determine whether the recipient is a Medicare patient. CMS states this will ensure the TH/OPO organ acquisition costs are more accurately applied to the Medicare program. CMS proposes changes to OPOs and their reporting requirements. Total usable organs for THs/OPOs will now be included into one of ten subcategories. CMS states these categories will more accurately explain various situations, including “organs transplanted into non-Medicare beneficiaries.” Organs not transplanted into Medicare patients are accounted to determine Medicare usable organs. Additionally, CMS further proposes policy changes on organ acquisition charges for kidney-paired exchanges in section k on page 25669 which include the tables below.
Toyon’s Take
CMS’s proposed changes are in effort to create a more accurate payment of the Medicare program’s share of organ acquisition costs. CMS plans to use their collection of data from transplant hospitals and organ procurement organizations to calculate their share of costs.
Recommendation: Toyon recommends the industry consider commenting on how this may not only impact current operations of your transplant services but future implications this may have on securing organs for use.
|
|
|
Medicare DSH Uncompensated Care (UC) Payments |
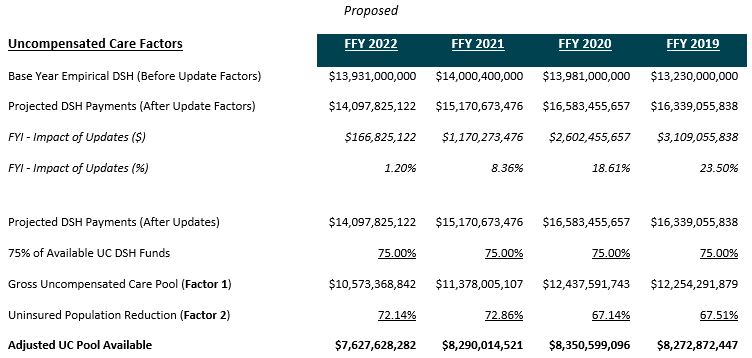
CMS proposes to decrease Medicare UC DSH payments by $662m, to $7.6bn in FFY2022. This decrease is primarily due to estimated DSH payments under the “empirical” method[1] - including data from the PHE - in the determination of “Factor 1.” Specifically, the $167m update[2] in the Factor 1 computation includes data from the PHE (notably discharges and Medicaid enrollment[3]) and is significantly less than prior year updates (e.g., $1.170bn in FFY2021).
|
|
|
[1] In the Factor 1 calculation, CMS first determines Medicare DSH payments in the absence of UC DSH payments under the ACA (section 1886(r)(1) of the Act). Data from the Office of the Actuary’s January 2021 Medicare DSH estimates, based on data from the September 2020 update of the Medicare Hospital Cost Report Information System (HCRIS) and the FFY2021 IPPS/LTCH PPS final rule IPPS Impact File.
[2] Updates include Market Basket (Update Factor component), ACA Payment Reductions (Update Factor component), Multifactor Productivity Adjustment (Update Factor component), Documentation and Coding (Update Factor component), Discharge Factor, Case-Mix Index Factor, and an Other Factor.
[3] The FFY2022 IPPS Proposed Rule updates include COVID-19 PHE Data, as follows:
“Discharge Updates for changes in the number of Medicare fee-for-service (FFS) inpatient hospital discharges. The figures for FFY 2019 and FFY2020 are based on Medicare claims data…The discharge figure for FFY2021 is based on preliminary data. The discharge figure for FFY2022 is an assumption based on recent trends recovering back to the long-term trend and assumptions related to how many beneficiaries will be enrolled in Medicare Advantage (MA) plans. The discharge figures for FFY2020 to FFY2022 reflect the estimated impact of the COVID-19 pandemic. The case-mix column shows the estimated change in case-mix (from 2018) for IPPS hospitals.
The case-mix figures for FFY2019 and FFY2020 are based on actual data adjusted by a completion factor. The case-mix figure for FFY2021 is based on preliminary data. The case-mix factor figures for FFY2020 and FFY2021 have been adjusted for the estimated impact of the COVID-19 pandemic. The FFY\2022 increase is an estimate based on the recommendation of the 2010 2011 Medicare Technical Review Panel.
The “Other” update shows the increase in other factors that contribute to the Medicare DSH estimates…In addition, the “Other” column includes a factor for the Medicaid expansion due to the Affordable Care Act…The ‘‘Other’’ column also includes the estimated impacts on Medicaid enrollment from the COVID-19 pandemic. We note that, based on the most recent available data, it is estimated that Medicaid enrollment increased by 2.9 percent in FFY2020 and will increase by an additional 1.2 percent in FFY\2021.”
|
|
|
In the Factor 3 distribution of each DSH hospital’s UC DSH allotment, CMS proposes one significant change, accounting for COVID-19, only using an average of two years discharge data (FFY2018 and FFY2019), rather than a three-year average that would include data from FFY2018, FFY2019, and FFY2020. CMS also proposes new trims to exclude rare cases hospitals do not have audited FFY2018 Worksheet S-10 data and are not currently projected to be DSH eligible.
Hospitals have 60 days from the date of public display of the FFY2022 IPPS/LTCH PPS proposed rule in the Federal Register (no later than 5 p.m. EDT on June 28, 2021) for comments. Related to proposed FFY2022 UC DSH payments, comments may be directed to [email protected] for issues concerning:
Toyon is in the process updating our national analysis to assist our clients with the evaluation of FFY2018 used for FFY2022 UC DSH payments. We will be providing this analysis over the coming weeks.
Toyon’s Take
Inclusion of certain PHE data
The proposed inclusion of discharges and Medicaid enrollment data from the PHE in the “Factor 1” calculation significantly lowers FFY2022 UC DSH payments. Toyon estimates at least an additional $1 billion in FFY2022 funding if CMS used the same discharge and other factor update in FFY2022 as it did in 2021.
Recommendation: Toyon recommends the industry consider commenting to freezing data prior to the PHE, allowing more time to evaluate national Medicare Uncompensated Care funding considering on-going COVID-19 healthcare issues.
Notably, in the FFY2022 IPPS Propose Rule, CMS notes in developing Medicaid expansion estimates, the Agency’s actuaries “assumed new Medicaid enrollees are healthier than the average Medicaid recipient and, therefore, use fewer hospital services”. Specifically, CMS cites the Office of the Actuary assumed per capita spending for Medicaid expansion beneficiaries at 78 percent of the average per capita expenditures for a pre-expansion Medicaid beneficiary. CMS further notes this same assumption was used for the new Medicaid beneficiaries who enrolled in 2020 and thereafter due to the COVID–19 pandemic.
New S-10 Cost Reporting Instructions for FFY2021 Cost Reports
- Shift to Short Term Hospital Services Only
- Split between patient coinsurance, copayment deductibles vs. other patient liabilities
- Clarification on the reporting of Implicit Price Concessions and Inferred Contractual Relationships
- New Reporting Tables for Charity Care and Bad Debt Information
In the FFY2022 IPPS Proposed Rule, CMS thanks stakeholders for their comments on the PRA package and states the Agency will respond to industry comments in a separate Federal Register document.
Recommendation: Toyon recommends CMS postpones its proposed instructions allow providers more time to adapt to the operational changes and prepare for the impact of these changes.
FFY2018 UC Cost and Source HCRIS Data
CMS used HCRIS data through February 19, 2021 for FFY2022 UC DSH payments in the FFY2022 IPPS Proposed Rule. The Agency notes its intention to use the March 2021 HCRIS for the FFY2022 final rule and the respective March updates for all future final rules. CMS also states it may consider the use of more recent data that may become available after March 2021, but prior to the development of the final rule, if appropriate, for purposes of calculating the final Factor 3 for the FFY2022 IPPS/LTCH PPS final rule.
Recommendation: Toyon recommends all hospitals verify audited FFY2018 S-10 UC cost is reflected in the FFY2022 IPPS Proposed Rule.
If not reflected in the FFY2022 IPPS Proposed Rule, it is recommended hospitals contact CMS to verify the agreed-upon FFY2018 UC cost audit amounts from WS S-10 will be used in the development of the FFY2022 IPPS Final Rule. Toyon will be assisting our clients with this exercise, and please contact Fred Fisher at [email protected] with any questions concerning S-10 uncompensated care for your hospital(s).
|
|
|
Empirical DSH - Section 1115 Waiver Days
The FFY 2022 Proposed Rule states Section 1115 days may be counted in the numerator of the Medicaid fraction only if the patient is eligible for inpatient hospital services under an approved State Medicaid plan that includes coverage for inpatient hospital care on that day or directly receives inpatient hospital insurance coverage on that day under a Section 1115 waiver. This excludes patient days for which hospitals receive payment from an uncompensated care pool.
Toyon's Take
This proposal contradicts recent court rulings and providers should expect waiver days to be closely reviewed during audit. Toyon recommends claiming these patients as a separate population on their own tab to reduce audit risk as any findings would be limited to similar patients.
Medicare Bad Debt
The FFY 2022 Proposed Rule requires State Medicaid programs to accept enrollment of all Medicare-enrolled providers and suppliers (even if the provider or supplier is not recognized as eligible to enroll but meets all Federal Medicaid enrollment requirements) for purposes of processing Medicare-Medicaid dual eligible claims for cost-sharing liability. State Medicaid programs must be in compliance for dates of service beginning January 1, 2023.
Toyon's Take
The “must bill” policy is still in place. This proposal should create additional opportunity for providers to claim Medicare bad debt on the cost report. CMS hopes this proposal leads to a reduction in the number of future bad debt appeals.
|
|
|
Other Rules, Transmittals, and Articles Recently Published |
Inpatient Psych Facility PPS FFY2022 Proposed Rule [CMS-1750-P]
(Display Copy available 4/7/2021; FR Publish Date 4/13/2021)
- Per diem base rate increase from $815.22 to $833.50.
- Total estimated payments to IPFs are estimated to increase by 2.3% or $90 million in FFY2022 relative to IPF payments in FFY2021.
- For FFY2022, CMS is proposing to update the IPF PPS payment rates by 2.1% based on the proposed IPF market basket update of 2.3%, less a 0.2 percentage point productivity adjustment.
Inpatient Rehab Facility PPS FFY2022 Proposed Rule [CMS-1748-P]
(Display Copy available 4/7/2021; FR Publish Date 4/12/2021)
- Standard payment conversion factor increase from $16,856 to $17,273.
- CMS is proposing the adoption of the COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) Measure to require IRFs to report COVID-19 HCP vaccinations in their facilities.
Long-Term Care Hospital PPS Proposed Rule [CMS-1752-P]
(Display Copy available here 4/27/2021; FR Publish Date 5/11/2021) – Published as part of the IPPS Acute Care Hospital Proposed Rule
- LTCH-PPS payments expected to increase by 1.4% or $52M.
- LTCH PPS payments for FFY2022 for discharges paid the site neutral payment rate are expected to increase by 3 percent. CMS estimates that discharges paid the site neutral payment rate will represent approximately 25 percent of all LTCH cases and 10 percent of all LTCH PPS payments in FFY2022.
Skilled Nursing Facility FFY2021 PPS Proposed Rule [CMS-1746-P]
(Display Copy available 4/8/2021; FR Publish Date 4/15/2021)
- Increase in unadjusted Federal per diem rates of 1.3%
- CMS is proposing to rebase and revise the SNF market basket to improve payment accuracy under the SNF PPS by proposing to use a 2018-based SNF market basket to update the PPS payment rates, instead of the 2014-based SNF market basket.
|
|
|
Should you have further questions about these changes and wish to discuss them, please contact the [email protected]. |
|
|
TOYON ASSOCIATES, INC. | toyonassociates.com |
|
|
|
|
|
|
|