What's the Yoga Therapy to Recover from Scapular Removal Surgery?
Holly: Hi Martin! I am in need of your geek expertise:) I have an amazing student who had a huge tumor removed from his shoulder & has rebounded from a long battle with cancer. To get the tumor they had to remove his shoulder blade. He still has the top of his scapula, but that's it. Do you have any yoga therapy suggestions for him? He wants to do vinyasa yoga & does so using a block for support in down dog. He can't get his arm much higher than his heart at this point. Thanks Martin! I hope you are having a wonderful fall:)
Martin: Wow, Holly. This is a very interesting case. First and foremost, kudos for the courage of your student and I wish him continued recovery. The shoulder blade is critical in providing stability for the shoulder joint, elbow, wrists & hands.
Holly: It intrigued me too! Just to watch how he modified throughout class was so impressive! You are more than welcome to use this for Therapy Geek. I look forward to seeing what you can come up with! Thanks Martin!
Martin: Great Holly. Let's start with the anatomy.
Scapular Anatomy
The scapula is a thin, elegantly sculpted blade with a convex anterior curve that is shaped to fit the back of your rib cage. Its only bony  attachment to the axial skeleton is to the sternum via the clavicle. Your arms go along for the ride as your scapula glides over the back of your ribcage pulled by a full complement of stabilizer muscles. Your scapula is relatively thin from front to back but has ample structural integrity to withstand the forces of push and pull it must endure. It is a floating platform that gives a bony landing for the forces developed in the arms during weight bearing and when placed properly, it can successfully transfer those forces to the rib cage.
attachment to the axial skeleton is to the sternum via the clavicle. Your arms go along for the ride as your scapula glides over the back of your ribcage pulled by a full complement of stabilizer muscles. Your scapula is relatively thin from front to back but has ample structural integrity to withstand the forces of push and pull it must endure. It is a floating platform that gives a bony landing for the forces developed in the arms during weight bearing and when placed properly, it can successfully transfer those forces to the rib cage.
Muscles attach to almost every surface of the scapula the scapula so the loss of any portion of it is serious.
If your student has only the top of his shoulder blade, he must be missing most of the blade below the scapular spine (SS). You can find your scapular spine if you reach over your opposite shoulder and rub your fingers up and down on your shoulder blade. The horizontal bone structure you feel is your SS. I am assuming for this article that your student still has SS and everything above it.
What Muscles are Compromised?
There is a significant amount of the rotator cuff muscle mass that originates below the SS. If part of the scapula below the SS is removed, many attachments have been compromised.
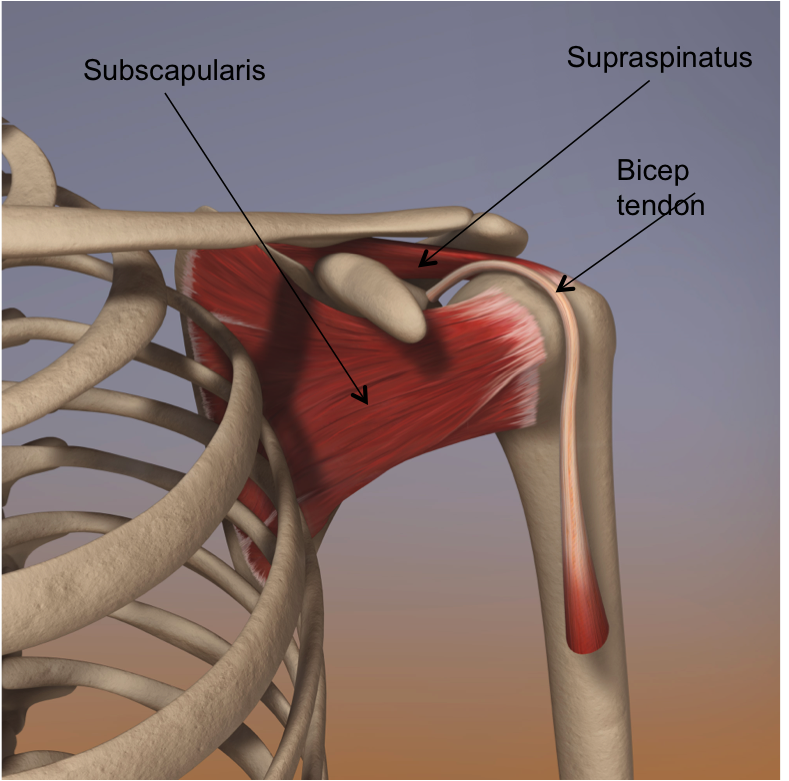
Here are the rotator cuff muscles that would be compromised by such a surgery. On the anterior scapula is the subscapularis. It uses most of the anterior scapular face as its origin. It inserts into the lesser tubercle humeral head.
On the posterior scapula two cuff muscles originate below the scapular spine. Infraspinatus originates on most of the scapular face below the SS. Teres minor originates from the lateral edge of the scapula below infraspinatus.
Several scapular stabilizer muscles attach below the SS and thus would be  compromised by the surgery. The rhomboids insert on the medial edge of the scapula and originate on the spinous processes. Rhomboid minor might survive intact since it inserts mostly above SS. However, the insertion of rhomboid major is completely below SS. Rhomboid major would be sorely missed for its contribution to shoulder stability.
compromised by the surgery. The rhomboids insert on the medial edge of the scapula and originate on the spinous processes. Rhomboid minor might survive intact since it inserts mostly above SS. However, the insertion of rhomboid major is completely below SS. Rhomboid major would be sorely missed for its contribution to shoulder stability.
Another critical stabilizer, serratus anterior (SA) inserts along the entire medial border of the scapula from top to bottom. Most of SA would be compromised in the surgery. Two other muscles attach to the inferior angle of the scapula: Teres major and latissimus dorsi (not shown). Both have the ability to move and stabilize the scapula when present.
The Problems
As you can see there is a LOT going on with the scapula and its partial removal can have major consequences. Let's examine some important problems.

-
When the scapula is anchored in its optimal position on the back of the ribcage, it protects all downstream joints (shoulder, elbow, wrist and the joints of the hand). The protection mechanism depends upon good contact between the back of the ribcage and the scapula. With most of the scapula missing, your student has nothing to anchor to his ribcage. Therefore most of his downstream joints are at risk.
-
The scapula must be stable on the ribcage for safe weight bearing work with the arms. With much of the attachment area for the scapular stabilizer muscles gone, it will be much more difficult to stabilize.
-
The rotator cuff muscles play a major role in stabilizing the shoulder joint or glenohumeral (GH) joint. With much of the blade removed, these cuff muscles have lost their origin and will be severely compromised in their ability to stabilize the GH joint. The risk of shoulder dislocations and rotator cuff tearing increases.
-
Two major stabilizers that are compromised are the rhomboid major (RM) and serratus anterior (SA). RM draws the scapula to the midline (retraction) and SA pulls the scapula away from the midline (protraction). RM is also an important downward rotator of the scapula that draws the bottom tips to the midline. RM is the ONLY muscle with this capability and its loss cannot be replaced. SA would be compromised in its ability to upwardly rotate the scapula. The trapezius should still be able to upwardly rotate because it inserts along the scapular spine.
This Student's Case
There are likely a lot of alignment issues as your student struggles to practice yoga in the wake of his surgery. For simplicity's sake, let's pick two major issues and look for therapies.
-
Issue #1: You mentioned that he has limited range of motion (ROM), ie, he cannot get his arms much higher than his heart. That is probably due to the loss a lot of upward rotation capacity. It is necessary rotate the scapula upwardly to freely take the arms overhead. The serratus anterior pulls the bottom tip of the scapula laterally to create rotation. Your student has no bottom tip to pull upon.
- Issue #2: I'm guessing that your student will have lot of trouble keeping the head of his humerus back (HHB) as well for several reasons.
- Usually the rhomboids can retract the bottom tip of the scapula to help with HHB. With no bottom tip, he cannot retract.
- The posterior rotator cuff muscles (infraspinatus and teres minor) pull the head of the humerus to the back of the shoulder socket. With most of their origin removed they will have much less power for this action.
- The anterior muscles (pectoralis major & minor) are likely contracted post surgery since he is likely keeping the head of the humerus forward. They will need to be stretched.
How to Help
Let's take each issue separately.
-
Issue #1: Limited ROM overhead. I recommend a 2-pronged approach.
-
Issue #2: Difficulty keeping the head of the humerus back (HHB).
-
Basically, his only remaining tool to keep HHB is his trapezius. The good news is the traps insert along the scapular spine which he still has. The bad news (sort of) is that his brain has had a lifetime to operate his traps in conjunction with the other stabilizers. Now, the traps are on their own. The really good news is that the brain is incredibly plastic and can be reprogrammed to its new task. Here's an exercise for that.
-
 |
| � 2010 Witold Fitz-Simon |
-
Have him lie on his back with his arms out to his side, palms face up.
-
Have him bend his knees, with his feet off the floor and inhale.
-
On exhale have him draw his injured shoulder down to the floor. This will activate whatever muscular capacity he has for HHB.
-
On exhale have him twist at the waist to take his knees away from the injured side. Go only as far as he can keep his shoulder down.
-
Inhale his knees back up. Exhale and repeat.
As long as your student is willing and motivated to work, he should make progress. I am always inspired when a student shows courage and determination like this. And I'm proud of teachers like you willing to help the student find a way. Good for you, Holly and happy Geeking.
With Love,
Martin






 teaching skills, coupled with a deep understanding of the principles of yoga therapy, will give you the confidence you need to be of real help for your students. You will know how to keep them safe in your class and even how to use your class to help them heal. In addition, you will gain the knowledge and skills to help you establish your own private yoga therapy practice. If teaching yoga and yoga therapy are your thing, this is the training for you.
teaching skills, coupled with a deep understanding of the principles of yoga therapy, will give you the confidence you need to be of real help for your students. You will know how to keep them safe in your class and even how to use your class to help them heal. In addition, you will gain the knowledge and skills to help you establish your own private yoga therapy practice. If teaching yoga and yoga therapy are your thing, this is the training for you.

