|
Serotonin syndrome (SS) was first described in the 1960s but gained attention in 1984 following the tragic death of Libby Zion due to a fatal drug interaction involving multiple serotonergic drugs. The syndrome is primarily the result of drug interactions between multiple serotonergic drugs and less commonly from an overdose of a single serotonergic agent. It develops rapidly, often within 12–24 hours of starting a new drug that increases serotonin and is characterized by a spectrum of clinical manifestations.
Serotonin syndrome arises from excessive serotonergic activity in the central and peripheral nervous systems, resulting in elevated intrasynaptic serotonin levels. Proposed mechanisms include increased serotonin synthesis, reuptake inhibition, impaired metabolism via monoamine oxidase, enhanced serotonin release, and direct stimulation of serotonin receptors. It is thought to be primarily driven by overactivation of 5-HT1A and 5-HT2A receptors.
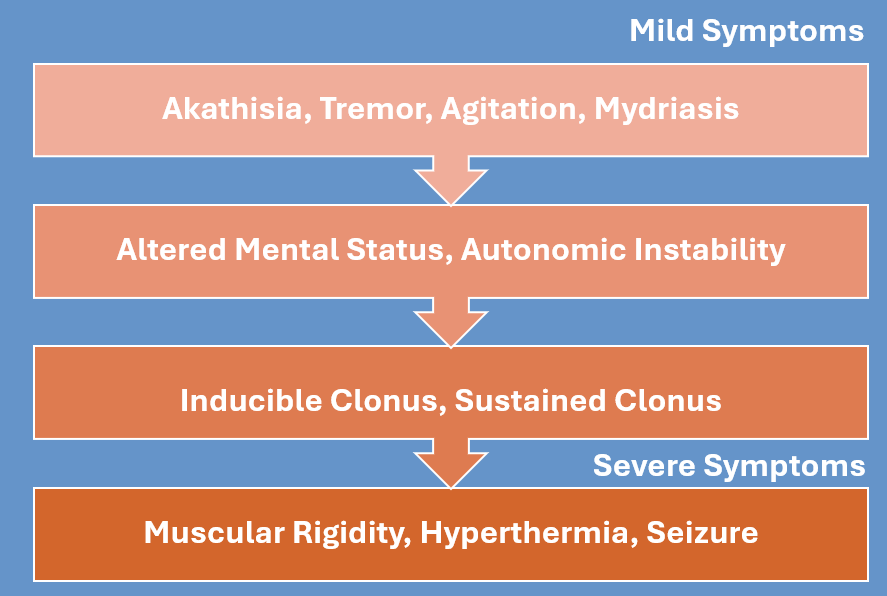
The clinical triad of symptoms in those with serotonin syndrome include mental status changes (agitation, delirium, seizures, etc.), sympathetic hyperactivity (tachycardia, hypertension, fever, etc.), and neuromuscular abnormalities (hypereflexia, clonus, akathisia, etc.) (Boyer & Shannon, 2005).
No lab tests are available to confirm the diagnosis, however a few criteria have been proposed. In the Hunter Criteria model the presence of clonus combined with the use of a serotonergic agent plays a critical role in supporting the diagnosis. A limitation of this model, however, is its potential to overlook mild cases of serotonin syndrome (Dunkley et al., 2003). Due to this limitation consider contacting your local poison control center at 1-800-222-1222 for all cases, especially those in whom you have a high suspicion of toxicity, but who do not meet Hunter Criteria.
It is important to obtain patient history and medications to rule out other diseases/causes that may present very similarly, including withdrawal, sepsis, meningitis, sympathetic storm, etc.
The first step to take is to remove the offending agent(s) that are contributing to the abundance of serotonin. The overall goal of therapy is symptom relief using cooling measures and benzodiazepines. In mild and moderate cases, benzodiazepines are usually sufficient, and can help with agitation, hypertension and tachycardia. Few studies have shown the use of cyproheptadine, a first-generation antihistamine with anti serotonergic activity, however, there are no randomized controlled studies to support its effectiveness. Additionally, cyproheptadine is given PO only, and takes hours to reach peak plasma concentration.
In most cases of serotonin syndrome once the offending agent is discontinued, resolution of symptoms occurs within 24 hours (Boyer & Shannon, 2005; Graudins et al., 1998).
|