|
Is Your PDPM Coding SPEECH-tacular?
The SLP case mix has so many things going on! Which means there is lots of opportunity to showcase your assessment and IDT skills! But it can also mean lots of opportunity for errors - both by way of overlooking something that’s there or taking credit for things that aren’t supported. Here are a few places where a little attention can go a long way.
Identifying Cognitive Impairment
The VA says that between 45 and 65% of patients in skilled nursing facilities have cognitive impairments. If your numbers seem unusually low (or high) compared to that then you may need to boost your assessment skills for the BIMS. Remember that if any cues or prompts are given, the score goes down – the interview is scripted and timed; we are not to deviate from the instructions or the prompts (note that this is different from the PHQ9 where you are allowed to ask the patient to expand or facilitate more detailed responses). This is very explicit in the instructions, but it’s so easy for us to fall in the habit of helping but not realizing we’re helping! Make sure your interviewers are savvy here – review the administration guidelines starting on page C-5 of the RAI manual or the BIMS guide on the Portal for detailed instructions.
Altered Texture Diet *IMPORTANT UPDATE HERE! *
If your facility follows the IDDSI diet level protocols, we have good news for you! We have confirmed directly with IDDSI (The International Dysphagia Diet Standardization Initiative) that the diet texture, “Level 7-Regular, Easy to Chew,” can be coded as an altered texture diet on the MDS.
That’s the good news! The bad news is that a common mistake we make is taking credit for the altered diet when it’s been ordered after the lookback period. An altered diet only counts for PDPM if it’s ordered during the lookback period, so make sure your team is watching those dates closely and communicating them to your SLP and/or RD for prompt assessment of texture needs.
One final piece of altered texture guidance: never place a patient on an altered diet without a documented reason to do so. There is no basis to downgrade diets routinely on admission. An altered diet is a medical intervention and creates a restricted environment. Altering diet textures without a documented reason can create survey issues in addition to prompting potentially thorny questions about billing practices.
Identification of Swallowing Problems
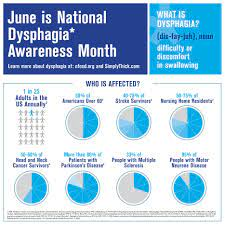
Around 40% of patients in SNFs have some type of swallowing problem according to ASHA. Swallowing problems correlate directly to risk for malnutrition, dehydration, skin breakdown, poor response to medical treatment or physical rehabilitation and decreased quality of life. Don’t let them go unmanaged! The SLP doesn’t have to be the one to see or document them – there are many, many, many screening tools that can be used by nurses and other professionals to identify and document these common problems. But remember! Even though sometimes the presentation is mild, and the rules say that documentation of the problem only needs to occur once in the lookback for MDS purposes, most patients with swallowing problems require some degree of management, even if it’s only adaptation or compensation. It should not be a common occurrence that the problem is identified but not a thing needs to be done about it. In addition to potentially undermining you claim for payment, it is a potential survey issue to identify a problem but then not respond to it.
SLP Co-Morbidities
While some of these are very clear-cut (we’re just not likely to mis-code a ventilator!), a few need a bit of clarifying.
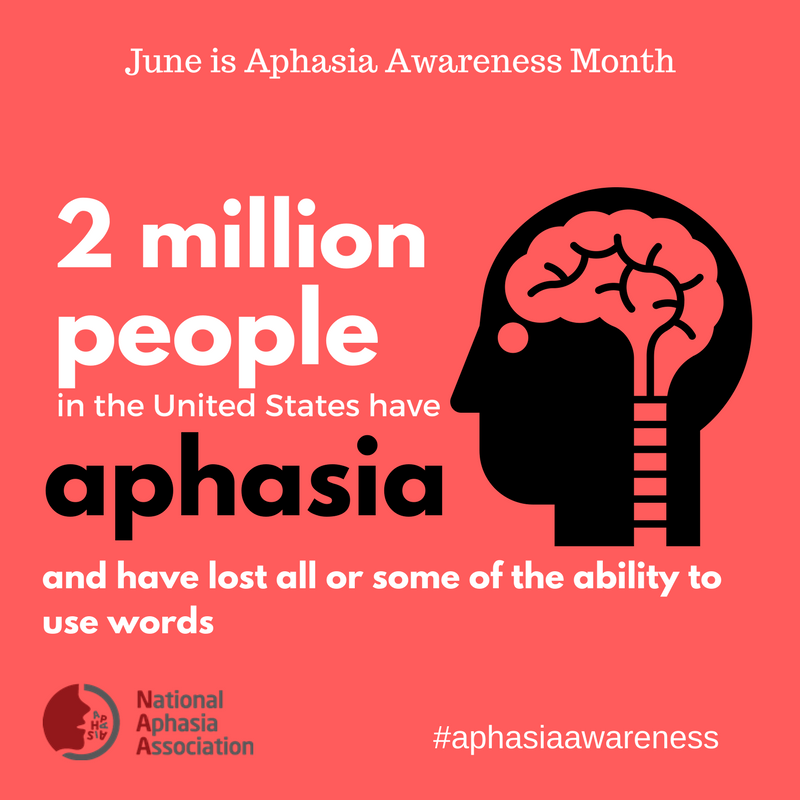
Aphasia, item I4300. Aphasia is a disruption of language due to damage to the language centers of the brain and encompasses impairments in word-finding, expression, and comprehension. I4300 can be checked when a diagnosis of aphasia of some type has been identified and confirmed by a provider (and when it is impacting the patient in some way – remember that this is a Section I item!). There are many types, here is a guide to proper diagnosis selection and coding:
o An aphasia diagnosis from the I69 ICD-10 series is only supported if the patient has had a CVA or has other physician confirmed cerebrovascular disease.
o Coding aphasia, R47.01 is supported when language disruptions exists from other neurological etiologies like traumatic brain injury, brain tumors or surgery.
o Coding Primary Progressive Aphasia (G310.01) is supported when a physician has diagnosed either PPA, Pick’s Disease or Progressive Isolated Aphasia.
o Coding Developmental Aphasia (F80.1/F80.2) is supported when the patient has a developmental disorder (eg: Down’s Syndrome, Autism Spectrum Disorder, Pervasive Developmental Disorder) when language impairments exist and can be identified distinctly from other intellectual disabilities.
o When language manifestations exist in the presence of global cortical disease or injury (e.g.: Alzheimer’s Disease, Parkinson’s Disease, ALS, delirium, encephalopathy or encephalitis) it is much, much more likely that the impairments are in attention, working memory and cognitive processing. While they may appear similar to aphasia in presentation, they are not aphasias diagnostically and standardized testing has limited ability to differentiate the conditions. The vast majority of patients who have these conditions are more properly diagnosed with R41.841, Cognitive Communication Deficit.
• Coding Dysphagia, Dysarthria, Apraxia, Fluency Disorder or Other Speech and Language Impairments following Cerebrovascular Disease (other or unspecified) is supported when those conditions are identified in the presence of a stroke, multi-infarct dementia, vascular stenosis, vascular dementia or unspecified cerebrovascular disease; but are not supported when the underlying etiology is Alzheimer’s Disease, Parkinson’s Disease or other non-specific dementias.
Finally, you may have noticed a few links in the newsletter. There is a bounty of helpful SLP Case Mix tools located on the PDPM Tools page on the Portal. Click here and scroll down to SLP Case Mix tools to see what’s available to you!
Special thanks to Elyse Matson, SLP, for organizing and often developing the incredible SLP case mix tools we have!
|