Brian Zikmund-Fisher, PhD
Editor-in-Chief
|
Ellen G. Engelhardt, PhD
Deputy Editor
|
|
by
Brian Zikmund-Fisher
, PhD; University of Michigan
In this issue of the Newsletter, I want to highlight SMDM Trustee
Ava John-Baptiste
’s commentary, “Social Policy and Health: What is Our Role?” In it, Ava reminds us that our work within SMDM exists within the much broader context of the well-known social determinants of health. She prompts us to reflect on whether MDM work can be improved through considerations of these social determinants and to consider when advocacy on such issues is appropriate.
As someone whose primary appointment rests in a school of public health, I have conversations about social determinants on a nearly daily basis with my students and colleagues. Yet, it is also true that those conversations have had only limited impact on my research trajectory. I thank Ava for prompting each of us to consider our role in addressing the systemic inequalities and structural barriers to health that exist globally, nationally, and locally, no matter where you are.
I also encourage members to read SMDM President
Heather Gold
’s letter, which encourages members presenting at our upcoming Annual Meeting in Portland, Oregon, to consider being innovative in the design of their posters and presentations. As a #scicomm person who believes that the value of SMDM work is dependent on how clearly and effectively we communicate it, I’m happy to encourage all SMDM members to focus not only on doing good work but on also communicating it well.
Other highlights of this issue include:
- Mark Liebow's update on the current state of health-related bills in the U.S. Congress.
- A commentary from Infectious Disease Modeling Interest Group co-chairs Eva Enns and William Wong highlighting the way SMDM can help improve the disease modeling used to inform policy decisions.
- Ankur Pandya challenges us to consider the value of teaching MDM topics online and to consider whether we should build our own online content or point to others’.
- Deputy Editor Ellen Engelhardt’s summary of the findings from the Spring Scientific Issues in SMDM Poll, which finds that SMDM members appear highly interested in international collaboration yet clearly see significant barriers inhibiting such efforts.
In addition, check out our Summer Poll, which focuses on our thoughts on patient participation in research. This topic seems particularly timely, given that SMDM has a new PCORI grant to bring many stakeholders (including patients) to our upcoming meeting. Please take 2 minutes right now and participate!
Looking forward to seeing many of you in a few months in Portland!
|
|
|
|
|
|
Effective Scientific Communication (#SciComm) and Other Musings from the SMDM President
|
by
Heather Taffet Gold,
PhD; New York University School of Medicine
It’s been an exciting time for the Society for Medical Decision Making, as you’ll see with this update. From plans and ideas for our October meeting, to our new fellowship program, to new initiatives, we are busy year-round to make our organization relevant and engaging.
The North American meeting, being held in Portland, Oregon, from October 20-23, 2019, will be a terrific forum for learning new science, sharing ideas about the field, and networking with colleagues. Our meeting chairs have been hard at work putting together an incredible program and raising funds to support their efforts. A new grant from the Patient-Centered Outcomes Research Institute will support involvement of a wide variety of stakeholders at the meeting, including patients, clinicians, health system leaders, and payers, along with other meeting activities. Be sure to register for our Portland meeting by September 25, 2019, to get the early discount registration rate.
If you’re presenting a poster, I encourage you to consider novel formats and thoughtful design for your poster, rather than a large “print-out” of a scientific article or standardized template with too much text and too little white space. I have been thinking a lot about data visualization and effective communication, which are also related to the
visual abstract
.
Twitter led me to
this video
for a new poster format, which you might consider adapting. Note that not everyone knows how to scan a QR code, so adaptation rather than pure adoption might work better. (And adapting it might be more effective as
addressed here.
Also
see this.
This blog
also has interesting poster ideas, with links to pages that help us think about effective ways to present research findings. Essentially, keep it simpler than you think you should, focusing on a clear message.
The goals behind these innovative poster presentations hold for oral presentations, too. Because you’re an expert in listening to scientific talks, you can use that expertise to inform your own delivery. Get to the point quickly, perhaps starting with your conclusion and polished take-home message, and then telling the story of your scientific process and findings. Be aware that the entire audience will not be paying attention completely the entire time – that is human nature. Keep slides simple using only the most essential elements, and if you aren’t going to explain something on the slide, delete it. There’s some helpful information in
this video
, even if it is for a longer session than typical SMDM oral presentations. If you think you might be nervous, then script your talk. And regardless of your level of experience, practice sufficiently so the audience feels confident in what you are saying.
As you may have heard, we have announced and launched our new SMDM Fellowship Program in Medical Decision Making with funding from the Gordon and Betty Moore Foundation. The four fellows range in research area and expertise and are
Eline Krijkamp
(Erasmus University Medical Center, The Netherlands),
Kyu Eun Lee
(Stanford University, California, USA),
Ruth Ndjaboué Njike
(Laval University, Canada), and
Rachel Pozzar
(Dana-Farber Cancer Institute, Boston, USA). All have mentors who are long-time SMDM members. The fellowship will support these early career researchers, develop their potential to influence clinical practice and health policy, and prepare them to thrive in the field of medical decision making. The fellowship will leverage SMDM’s strengths of 1) convening experts who are at the forefront of innovation in medical decision science and 2) building capacity to thrive in the field of medical decision making.
In other news, our Membership Committee developed a slide template you can use to advertise our scientific meetings. Keep your eye out for the announcement and slide. We welcome you to use the slide in your presentations, departmental newsletters, and/or website to spread the word of the groundbreaking science at our North American and European meetings.
Finally, be sure to vote! We have a strong slate of nominees for the SMDM Board of Trustees election, which is now open. Voting closes on Friday, August 23, 2019 at 3:00 PM Eastern Time. Please make sure to cast your ballot if you’re eligible.
|
|
|
|
The opinions stated in the following commentaries are solely those of the authors and do not reflect the opinions of the Society for Medical Decision Making or the author's institution.
|
|
|
|
Social Policy and Health: What is Our Role?
|
by
Ava John-Baptiste
, PhD; Schulich School of Medicine and Dentistry, Western University, Canada
The Society for Medical Decision Making is “an international, transdisciplinary group drawn together by our commitment to improving the health of individuals and populations.” Many describe SMDM as I do, as an intellectual home, at the leading edge of methodological advances in medical decision making research, whose members translate their work directly to improving health services, health policy and healthcare decision making.
Technological innovation and an explosion in medical knowledge have contributed to increased life expectancy. SMDM research aims to identify which of these technologies is effective, which are cost-effective and how best to communicate this information to clinicians, patients and policy decision makers.
However, I’m often humbled by the realities of the broader context in which we work to improve individual and population health. Health services are not the only determinants of health.
1. Income and Income Distribution
2. Education
3. Unemployment and Job Security
4. Employment and Working Conditions
5. Early Childhood Development
6. Food Insecurity
7. Housing
8. Social Exclusion
9. Social Safety Network
10. Health Services
11. Aboriginal Status
12. Gender
13. Race
14. Disability
SMDM members are leaders in health services research. Many of us conduct our work in ways that also address some of the other social determinants of health. But it’s worthwhile to think about how we can do better.
One way to do better is to look at our research increasingly through the lens of the other social determinants of health. For example, modelers can consider important sub-groups defined by poverty, race or other forms of social exclusion, to shed light on the value for money of addressing inequities. Decision aid developers can seek out socially excluded groups and consider their lived experiences.
Another way to do better is through advocacy. Many within SMDM have the public respect, leadership role and perhaps the responsibility to advocate for policies that can improve the health of individuals and populations. Some of these policies include criminal justice reform, climate change action, income redistribution, reducing gun violence, social inclusion and fairness policies, and advocating for high quality, publicly financed education. These policies may fall outside of our research portfolios, but the impact on population health is undeniable.
A recent,
high profile example
of the medical community using their position for advocacy occurred in the United States with the #thisisourlane movement. In response to disparaging remarks from the National Rifle Association (NRA), the medical community rallied around #thisisourlane, creating a high-profile Twitter trend that was covered extensively by the media. Certainly, the goal of #thisisourlane is to advocate for research on gun violence. But the way in which the medical community entered the debate, it is clear they were also using their voices in a political way to counteract the NRA.
Influencing social policy is difficult and some would consider it inadvisable for academic researchers. What do you think? How should we act; individually on election night, through individual political advocacy, or collectively using our positions to influence public policy and effect social change in order to improve public health?
For those SMDM members who are already making contributions to improve health in other social domains, I would love to hear from you and learn more about what you are doing. Perhaps we can continue this discussion at the annual meeting, in the form of a social policy and health interest group.
|
|
|
|
|
|
by
Mark Liebow
, MD, MPH; Mayo Clinic
The House of Representatives is moving faster on appropriations than the Senate is. The House passed the Labor-Health and Human Services appropriations bill June 19. You can find details
here
.
The appropriations bill includes $41.1 billion for the National Institutes of Health (NIH), an increase of $2 billion above the 2019 enacted level and $6.9 billion above the President’s budget request. The Centers for Disease Control and Prevention would get $8.3 billion, $938 million above the 2019 enacted level and $1.7 billion above the President’s budget request. Instead of moving the Agency for Healthcare Research and Quality (AHRQ) into the NIH with no new money, there would be $358 million for AHRQ, an increase of $20 million above the 2019 enacted level. Other research agencies are getting comparable increases.
The House passed another package of appropriations bills on June 25. VA Medical and Prosthetic Research would get $840 million, $61 million above the FY 2019 enacted level and $78 million above the budget request. The National Science Foundation would get $8.64 billion, $561.14 million above the fiscal year 2019 enacted level. Research and related activities are funded at $7.1 billion, $586.3 million above the current level.
However, the Senate will not consider its appropriations bills until July or even September. That’s because while the House’s appropriations bills were passed assuming the sequestration caps that would hold down discretionary domestic spending will be lifted, the proposal to lift them is still being negotiated between the House, the Senate, and the White House. As a result, the Senate is waiting until whether the caps will be lifted to decide what it will appropriate.
As usual, a conference committee will need to reconcile House and Senate appropriations amounts when they differ, the conference committee report will need to pass the House and Senate, and the President will need to sign the appropriation bill(s) before money can be spent. If this is not done by September 30, the House and Senate will have to pass a bill (a “continuing resolution”) that the President signs to permit these agencies to continue spending money, typically at or near Fiscal Year 2019 levels, until a appropriations bills for the rest of the Fiscal year is adopted.
The Patient-Centered Outcomes Research Institute (PCORI) was authorized for nine years by the Affordable Care Act (ACA) in 2010, and the funding for it was part of the ACA authorization. Unless PCORI is reauthorized by September 30, it will begin to shut down, though current funding will be protected. It’s unclear whether the Institute will be re-authorized, though there are growing efforts in Washington to make that happen, because its creation in the ACA may make it poison in the Republican-controlled Senate and in the White House.
Ned Sharpless, M.D. remains acting Commissioner of the FDA. When this was written, no one had been nominated for the Commissioner position. However, Sharpless is rumored to be in the running for that along with a Harvard dermatologist and a M.D. Anderson physician.
|
|
|
|
|
|
Infectious Disease Modeling Interest Group
|
by
Eva Enns
, PhD and
William W.L. Wong
, PhD; SMDM Infectious Disease Modeling Interest Group co-chairs
There is growing and renewed interest in infectious disease modeling to inform policy decisions. Models are needed to address optimal responses to emerging infectious diseases, such as Ebola or Zika viruses, as well as the re-emergence of vaccine-preventable diseases, like measles. There are also questions about how to allocate limited resources to address ongoing challenges posed by chronic infectious diseases, such as HIV and hepatitis C. Many of these policy questions require modeling disease transmission, which can pose unique modeling challenges.
The Infectious Disease Modeling Interest Group has a broad focus in infectious disease modeling encompassing all areas of infectious diseases ranging from directly transmitted infections (contact, airborne) to sexually transmitted infections and vector-borne infections. This Interest Group brings together SMDM members with an interest and/or expertise in infectious disease modeling, particularly in dynamic disease modeling to provide opportunities for intellectual exchange, research collaboration, and networking.
Each year, the Infectious Disease Modeling Interest Group hosts an in-person meeting during the SMDM annual North American meeting. In past meetings, we have had guest speakers describe infectious-disease specific software platforms and projects; consulted with attendees about best ways to address infectious disease modeling challenges; and discussed strengths and weaknesses of different infectious disease model structures in addressing specific classes of policy questions.
If you are interested in infectious disease modelling, we invite you to join the group in SMDM Connect to receive latest news from the group and get connected with our network of researchers who specialize in infectious disease modelling.
|
|
|
|
|
|
What is the Value of Teaching MDM Online?
|
by
Ankur Pandya
, PhD; Harvard T.H. Chan School of Public Health
Online learning, an increasingly important option in higher education, was a major topic discussed at our last Teaching MDM Interest Group gathering in Montreal at #SMDM18. We concluded that online teaching modules could be important complements or substitutes for our current, in-person SMDM teaching activities.
But, before taking the full leap into online teaching, the key question we should be asking is: what is the value of teaching medical decision making concepts online?
I searched the education literature for reviews or rigorous evaluations of online learning modules and did not find any decisive evidence for (or against) the value of online learning compared to in-person short courses. I even reached out to the
Twitterverse
and came away mostly empty handed.
Intuitively, online learning offers greater flexibility for students and perhaps faculty (assuming they have access to the necessary technology) to participate in the education process. This could be especially important for teaching medical decision making to individuals living in remote areas and/or with significant schedule constraints. On the other hand, I hypothesize that the per-student quality of learning is generally better in person. There are data showing that most students who start online modules don’t get very far before stopping.
A related extension of the primary question is: should SMDM members be involved in creating new online teaching materials, or simply point interested students to existing materials? For example, a Google video search for “cost-effectiveness analysis” leads to some online modules, although the quality of these videos is variable. ISPOR has online educational webinars for many of the topics we research (e.g., disease modeling, economic evaluation, patient preferences); however, many of these resources are gated (i.e., restricting viewing to ISPOR members).
The stylized figure below shows one way we can conceptualize these tradeoffs. The figure shows four possible options (including staying with current SMDM teaching activities) and possible costs and effects (MDM learning) for each option. Like an incremental cost-effectiveness analysis, the optimal choice among the four options will depend on the relative value of each upgrade (i.e., the slopes of the dotted lines) and the total budget that we are willing to spend on teaching MDM.
Join the Teaching Interest Group meeting at #SMDM19 in Portland to continue this and other conversations!
|
|
|
|
Ellen G. Engelhardt, PhD
Deputy Editor
|
|
Results from the Spring 2019 Scientific Issues in MDM Poll: Why international research collaborations are or are not happening
|
by
Ellen G. Engelhardt
, PhD; SMDM e-newsletter Deputy Editor
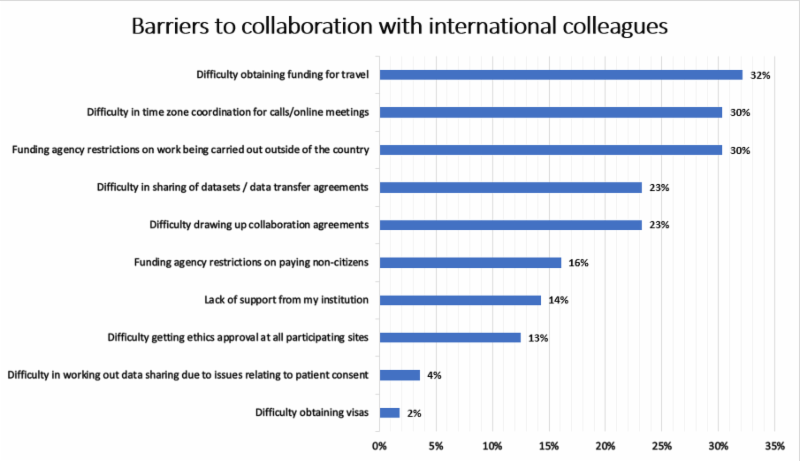
To what degree are international collaborations in research a common phenomenon among SMDM members? In the Spring 2019 poll, we explored your views on the value of international research collaborations and the key barriers that researchers in your field face that may be limiting such collaborations.
In total 56 SMDM members took part in the poll, thank you! Respondents identified their primary work in the SMDM subfields as follows: Health Services Outcomes and Policy Research (35%), Decision Psychology and Shared Decision Making (33%), Applied Health Economics (18%), Quantitative Methods and Theoretical Developments (8%) and Patient and Stakeholder Preferences and Engagement (4%).
International collaborations appear to be part of most respondents’ professional lives, as 77% (n=43) of respondents reported having carried out research in collaboration with international colleagues. Those who reported having international collaborations, indicated that these collaborations were mainly with researchers from North America (33%) and Europe (32%), but about one in ten (also) had collaborations with researchers from South America, Africa, Asia and Australia. Irrespective of whether they had experience with international collaborations, 69% of respondents indicated that they are likely to pursue collaborations in the future, whereas 21% indicated that they were unlikely to do so.
|
The barriers experienced by respondents were mainly related to funding, coordination across time zones and data sharing (see Figure 1). Most frequently perceived barriers related to securing funding to carry out the work once a promising partnership has been identified, but other issues listed by respondents included not having funding to attend conferences to make connections with researchers from other countries and to set up collaborations. SMDM members appear open to international collaborations. However, significant barriers, particularly in terms of funding, need to be overcome to enable more international research partnerships to occur.
|
|
|
|
|
|
SMDM 41st Annual Meeting
Many Views on Value
October 20 - 23, 2019
Portland, Oregon
|
Meeting co-chairs:
Karen Eden
, PhD,
Carmen Lewis
, MD, MPH and
Dan Matlock
, MD
This year's Annual Meeting will be held from October 20 - 23, 2019 at the DoubleTree by Hilton in Portland, Oregon, USA.
All health care decisions aim to optimize value; however, value is an elusive construct. First, “value” is both a noun and a verb, and it can relate to deeply held beliefs or a mathematical ratio of benefits and costs. The theme “Many Views on Value” rests on the idea that value is a function of the lens through which one sees the world. Inherent in this is an assumption that different stakeholders are necessary to understand the true value of any health care intervention. Members of SMDM are the academic leaders in understanding multiple stakeholder perspectives and in calculating value. The 2019 Annual Meeting aims to unite the robust behavioral science on perspectives with the rigorous analytical science of value.
The Keynote speaker is
Paul Slovic
, PhD. Dr. Slovic will give the Keynote Address on Monday, October 21 at 8:30 AM on The More who Die, the Less We Care: Confronting the Deadly Arithmetic of Compassion.
Visit the 41st Annual Meeting Homepage for more information. Meeting registration and the scientific program will be posted to the website in early August. We look forward to seeing you in Portland this October!
|
|
|
|
SMDM 2019 Board of Trustees Election: Voting is Now Open!
All SMDM members in good standing as of June 1, 2019 are eligible to vote. Instructions for voting along with candidate biographies were e-mailed to all SMDM members in good standing. Reminder voting e-mails will be sent to all members who have not voted throughout July and August until the voting deadline. If you have any questions regarding voting, please contact
[email protected]
.
This year, SMDM members are electing a President-Elect, Vice President-Elect, Historian and 3 Trustees, one of whom will be designated as an International Trustee.
The process for electing the International Trustee is as follows:
- Among the nominees for the three Trustee positions, the Nominations Committee has selected two candidates who are eligible for the International Trustee position: Jesse Jansen and Hester Lingsma.
- Among the nominees who are eligible for the International Trustee position, the nominee with the most votes will be elected to that position.
- Of the remaining nominees, the two nominees with the most votes will be elected as Trustees of the Board.
2019 SMDM Slate of Officer & Trustee Candidates
President-Elect (3 year term; 1 to be elected)
Jeremy Goldhaber-Fiebert, PhD
Natasha Stout, PhD
Vice President-Elect (2 year term; 1 to be elected)
Beate Jahn, PhD
Robert Volk, PhD
Historian (5 year term; 1 to be elected)
J. Robert Beck, MD
Trustees
(3-year term; 3 to be elected)
Jesse Jansen, PhD (International Trustee Nominee)
Tara Lavelle, PhD
Hester Lingsma, PhD (International Trustee Nominee)
Ankur Pandya, PhD
Sze-chuan Suen, PhD
Davene Wright, PhD
An important benefit of your membership in SMDM is the privilege to vote for leaders to represent YOUR Society. Your participation helps to build and enhance the Society now and into the future. Results will be announced via e-mail to the membership the following week after voting closes.
Voting closes on Friday, August 23, 2019 at 3:00 PM Eastern Time.
|
|
Latest News From Your Fellow Members
|
Tanya Bentley
, PhD, recently started a nonprofit research organization called the Health and Human Performance Foundation (
www.HHP-Foundation.org
). HHPF conducts research and communicates findings on the effectiveness of breath-related solutions for optimizing human potential. By focusing on the natural human capacity for stress regulation, HHPF research identifies solutions that complement western medicine while aiming to reduce the reliance on pharmaceuticals. At this early stage, while awaiting 501c3 approval from the IRS, Tanya would love to connect with fellow SMDMers with shared research interests.
[email protected]
|
Danny van Leeuwen
published the 11th episode on a podcast series about young adults with complex conditions transitioning from pediatric to adult medical care. The podcast can be accessed through
https://www.health-hats.com/ya_transition/.
|
Donna Berry, PhD, RN
, has returned home to the University of Washington, Seattle, to reclaim her position as Professor in Biobehavioral Nursing and Health Informatics after a ten year appointment at the Dana-Farber Cancer Institute in Boston. She will remain part-time at Dana-Farber to mentor post-doctoral trainee,
Dr. Rachel Pozzar
.(
[email protected]
)
|
Alan Schwartz
was named Interim Head of the Department of Medical Education at University of Illinois at Chicago. (
[email protected]
)
|
|
|
|
What Are You Working On?
Connect and collaborate with your fellow members on their latest projects:
Decision Support Platform for Patients & Providers for Ventricular Assist Device Therapy
CORA (Cardiac Outcomes Risk Assessment)
is a user-friendly computer application designed to provide decision support to patients and providers who are contemplating ventricular assist device (VAD) therapy for severe heart failure. Features include: (1) Prognostic models for survival and several adverse events (including stroke, GI bleeding, RV failure); (2) a Decision tree based on guidelines published by American Heart Association (AHA) and International Society of Heart & Lung Transplantation (ISHLT); (3) a “synthetic interview” module for patients with a collection of video vignettes of patients and providers answering common questions; and (4) a decision tool to assist patients to navigate their treatment options as they reflect their personal preferences, values and beliefs. The origins of CORA date back to 2004, but in the past 4 years has undergone significant development thanks to funding from NIH/NHLBI. It is hoped that CORA will help achieve consensus among stakeholders, and optimize the deployment of VADs, such that patients most likely to benefit will be prioritized, while those better served with conventional, or palliative care will be spared from unnecessary risks of debilitating side effects. The overarching goal is to optimize outcomes by facilitating collaboration between patient, providers, and care givers – based on personalized prognostic data, and by weighing all the important decision criteria. Current collaborations include: Cornell University, University of Colorado, Allegheny General Hospital, University of Rochester, University of Pittsburgh. We always welcome new collaborators.
View an additional CORA resource
.
|
|
|
|
Here are the most recent job opportunities since our last newsletter. SMDM members can stay current on the newest opportunities in the Resources Section of
SMDM Connect
.
|
|
The SMDM Lifetime Contributors list acknowledges the SMDM members who have made contributions to the Annual Fund and
acknowledges donations and in-kind donations, received from October 2005 - July 1, 2019.
Our heartfelt appreciation goes out to everyone who has supported our Society!
|
|
Editor-in-Chief
University of Michigan
|
|
Deputy Editor
Netherlands Cancer Institute
|
|
|
|
|
|
|