|
Did you get a low rumble, somewhere in the lower bowel….
… at the sight of the NHS vaccination factory set up in Kent, dispensing MenB jabs …
… we’ve been here before. Ooooh, nooo!
Public health hasn’t disappeared. It still has offices, directors, committees and acronyms. It produces reports, dashboards and earnest strategies, but…
… here’s the uncomfortable truth…
… it no longer has the power to make much difference where it matters most.
Once upon a time, public health was serious business.
It dealt with infectious disease, vaccination, sanitation, smoking. Big, population-level risks. It had authority, expertise and importantly, a national voice.
Then Andrew Lansley, for no good reason anyone could fathom, more an afterthought, stuffed it up the back passage of the Town Hall. Moved PH into local authorities.
Deracinated from its home and culture...
... on paper, it might have made sense. Health is shaped by housing, education, transport, environment, so shove it over to local government.
In practice, public health became one priority among many. Competing with potholes, social care budgets, bin collections and fly-tipping. Funding squeezed.
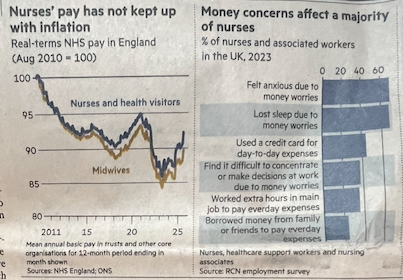
When PH moved to local authorities in 2013, there was a ring-fenced public health grant, however…
… between 2015/16 and around 2020, it was mugged. The public health grant fell by roughly £700m in real terms.
That’s about a 20-25% reduction per person, once inflation and population growth are taken into account…
… progressively defunded while being relocated to an already emaciated part of the system.
Influence over the NHS weakened, authoritative function fragmented, negotiated and often marginalised.
Now look at the problems we face.
Obesity isn’t about individual choice…
… it’s about a food industry that engineers products to be irresistible and cheap…
… social media isn’t just entertainment, it’s rewiring childhood, sleep, attention, morals and mental health.
-
These are not leaflet problems.
-
There are not logos on T-shirts.
-
These are the new, industrial-scale determinants of health.
Local public health teams;
-
cannot regulate global food-companies.
-
cannot redesign digital platforms.
-
cannot manage moral and ethical dilemma
-
cannot outgun the algorithm.
It's the law that changes behaviour; seatbelts in cars, smoking in the workplace, crash-helmets, health and safety, soft drink levies, SoMe regulation.
PH can do none of that. What are they left with?
Campaigns. Partnerships. Well-meaning initiatives. All worthwhile. All necessary. All hopelessly outmatched.
Meanwhile, the public-facing role has quietly shifted elsewhere. The NHS does the messaging. Health visitors, schools and community services do the engagement.
‘Wellness’ has emerged as the new language… pleasant, inoffensive and entirely without ownership, because…
…wellness lives everywhere…
... housing, jobs, education, environment… and ends up living nowhere in particular.
It’s into that vacuum, that public health has been sucked.
Responsible for everything. In charge of very little.
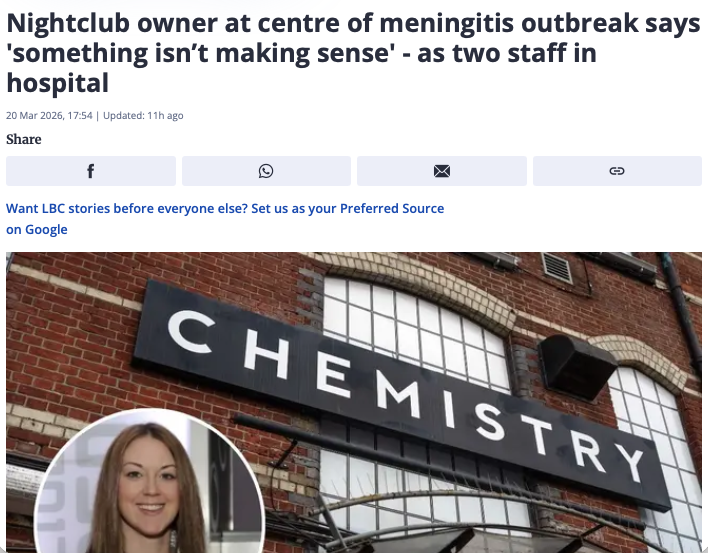
Then something happens. A meningitis outbreak, a new infectious threat.
Suddenly the system snaps back into focus.
Public health tracks, traces, advises, coordinates, predicts. It shows what it can do when given clarity and authority.
Which tells you something important.
The capability hasn’t gone.
The permission has.
What we have now is a kind of standby service. A fire brigade that’s excellent when the alarm sounds, but spends most of its time watching the wiring deteriorate and filing reports about the risk of sparks.
And the sparks are everywhere;
Ultra-processed food.
Sedentary lives.
Digital addiction.
Deepening inequality.
The drivers of ill health are no longer episodic. They are baked into how we live.
And, that requires power;
- national policy,
- regulation,
- taxation,
- cross-government action.
The kind of power public health no longer really has. So, we are left with a paradox.
-
We talk more than ever about prevention.
-
We invest less than ever in the means to deliver it.
-
We say we want a healthier population, but…
… we organise the system so that no one is truly responsible for making it happen.
Public health hasn’t gone. It’s has been hollowed out. Functions scattered. Authority diluted.
PH is a service with laryngitis; lost it’s voice.
When there’s an outbreak, we remember why it matters.
The rest of the time, it stands politely at the edge of the debate, watching, as the real drivers of poor health… commercial, social and now digital… roll on, unchecked.
We didn’t lose public health. We’ve forgotten about it.
If public health is to matter again, it must stop trying to run services and start calling the system to account.
PH has skills and talents that are under used. They must use those talents to become the ringmaster, the crusaders and the north star in the fight for a healthier nation.
Measuring, publishing and relentlessly pointing to where policy is making people ill. Refusing to let them be ignored.
Weaponise PH data in the fight for a healthier nation.
PH once stood centre stage. In the spotlight.
Now it’s like the ageing star at the Oscars.
Full of memories, but no new script.
|