February 28, 2020
The Out-of-Pocket Health News Digest:
Drug Pricing Special Edition
|
|
Below you will find an overview of drug pricing in the U.S. With this special edition, our hope is for students to understand the history and structure of U.S. drug pricing and current policy proposals.
This compilation is produced by the HPSA Education Committee: Sharoni Bandyopadhyay, Matthew Dunn, Payton Watt and Courtney Zott.
|
|
The History of U.S. Drug Pricing: A Timeline
|
|
1900-1910's
Drugs are relatively unregulated until the passage of the original Food and Drug Act, allowing the government to take action for the first time against mislabeled or “tainted” drugs.
1930's
The FDA’s authority is broadened and the seeds for its modern-day drug approval process are set with the passage of The Federal Food, Drug, and Cosmetic Act.
1940's
Continued deaths from tainted drugs spur the FDA to create good manufacturing practices (GMPs).
1950's
The Durham-Humphrey Amendment is passed, defining the drugs that cannot be used without a prescription.
1960's
Medicare (Part A and B), and Medicaid signed into law, creating a system of coverage which subsequently increases demand for health services and government spending. Medicare Part B covers a limited number of outpatient prescription drugs. Medicaid covers all outpatient prescription drugs.
1970's
Rapid escalation in overall healthcare costs.
1980's
The Drug Price Competition and Patent Term Restoration Act increases the availability of less costly generic drugs by allowing the FDA to approve applications for generic versions of brand-name drugs without repeating the research. The FDA allows prescription drug companies to advertise on TV, which causes prices to rise.
1990's
Series of proposed reforms to reduce regulatory burdens on pharmaceutical companies to spurn drug innovation. Section
340b
Drug Pricing Program is enacted, allowing hospitals to receive discounts on certain drugs.
2000's
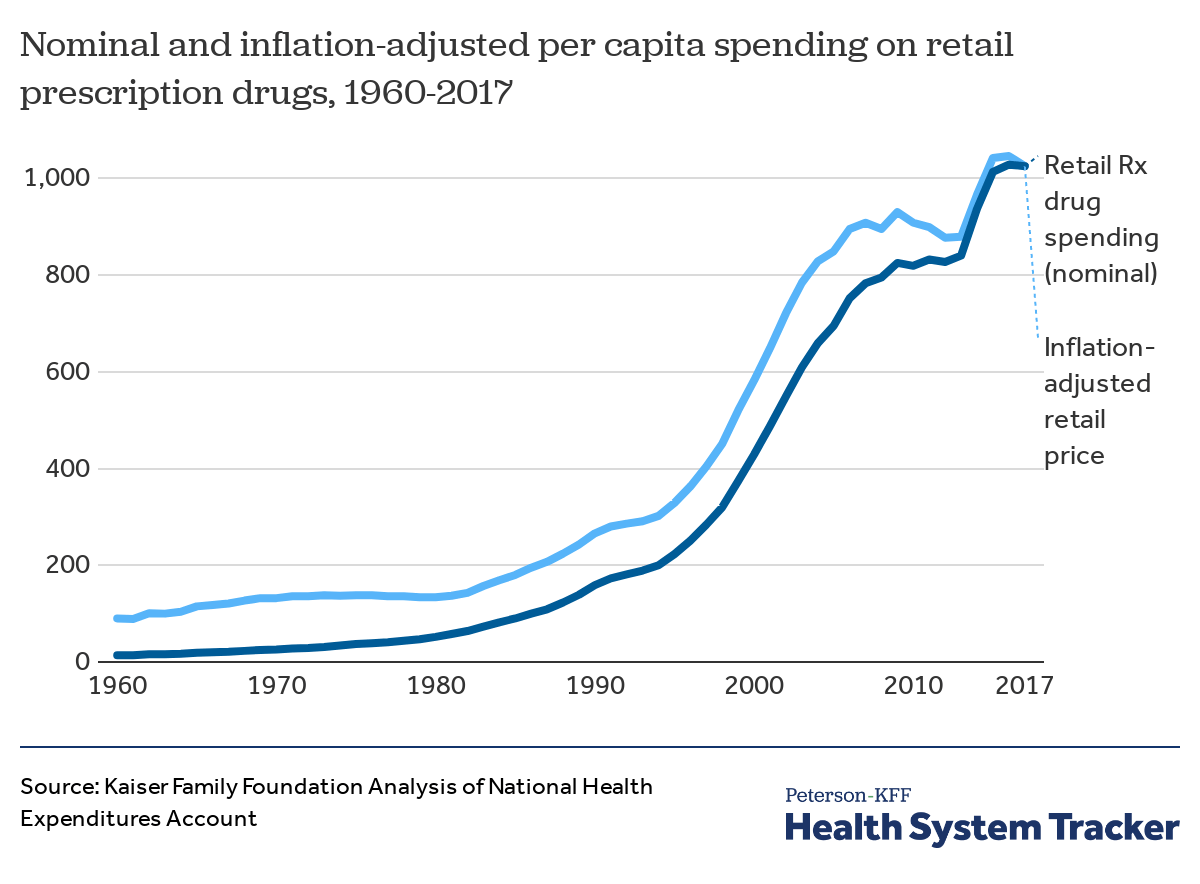
Drug prices triple. Prescription companies invent new types of prescription drugs-- advertised straight to consumers. U.S. government approves expensive drugs even if they are not much better than existing drugs. The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 establishes Medicare Part D which covers outpatient prescription drugs up to a certain point starting 2006, increasing the demand for drugs.
2010's
Patient Protection and Affordable Care Act does not directly address drug pricing despite dramatic increases in drug prices.
2020
Current drug pricing crisis leads to policy proposals and public outrage. Medicare Part D coverage gap
closes
.
|
|
The Role Of Pharmacy Benefit Managers - And Why They’re Under Scrutiny
|
|
Pharmacy benefit managers (PBMs) largely exist outside of public notice, but they play an important role in the distribution of drugs in the United States. These companies
negotiate with drug manufacturers
on behalf of public and private payers, with the goal of securing discount rates and rebates for drugs and ultimately reducing costs for the public. The role of PBMs also includes contracting with pharmacies to distribute drugs, and assuming administrative burden from the heath plans. PBMs are reimbursed for their services in two ways. First, PBMs pocket a share of the rebates from the manufacturers, while returning the rest to the payers. Second, PBMs invoice the health plans for drug and administrative costs.
However, PBMs have fallen under increased scrutiny for their presence in the drug distribution chain. In particular, there are concerns over the extent to which
PBMs profit
from collecting rebates, rather than passing more savings along to the public. There are also objections to a lack of transparency, given that much of their operations are out of public view.
In January 2019, the Trump Administration proposed a new HHS rule that would have imposed significant limits on the rebates drugmakers pay to PBMs. This proposal was
eventually rescinded
in July 2019, a decision likely impacted by strong pushback from insurers, hospitals, and the PBMs themselves. States may also be able to regulate PBMs, although this is uncertain for the moment. The 8th Circuit Court of Appeals recently struck down an Arkansas law governing reimbursement rates, but the
Supreme Court
granted the state’s appeal and will review the case in the current session. This case is expected to have far-reaching impact on the fate of PBMs in the U.S.
|
|
Current Policy Proposals Targeting Drug Pricing and Implications
|
|
Several policy proposals surrounding prescription drugs have emerged recently: the Democratic House’s
Elijah E. Cummings Lower Drug Costs Now Act
, the Republican Senate’s
Prescription Drug Pricing Reduction Act of 2019
, and the Trump Administration’s blueprint titled
American Patients First
. Many of the proposals address the same issues, but take different approaches. You can view comparisons between the bills from the Commonwealth Fund (
1
,
2
) and the
Kaiser Family Foundation
. Two of the most controversial proposals are implementing an international price index and enforcing inflation-based limits on drug pricing. An overview of the proposals for these two provisions and their implications are outlined below.
Reference Pricing:
H.R.3 is the only proposal that authorizes the government to negotiate drug prices with pharmaceutical companies, which is currently cannot do. The bill includes a provision that allows the Secretary of Health and Human Services to negotiate drug prices for at least 25 of the 125 most expensive prescription brand-name drugs that lack generic competition, as well as insulin. This “maximum fair price,” would be determined through an international price index, capping the cost at no more than 120% of the average price of the following countries: Australia, Canada, France, Germany, Japan, and the U.K. For drugs that do not have an average international market (AIM) price, the price cannot exceed more than 85% of the average pharmaceutical manufacturer’s (APM) price. Both public and private insurers would be able to purchase drugs for this negotiated price. Pharmaceutical companies that fail to negotiate would be fined 65% to 95% of the prior year’s revenue for the specific medication. Trump outlined a similar proposal in his blueprint, but without an enforcement mechanism to ensure negotiation.
Negotiating drug prices to 120% of the AIM price would reduce the cost of drugs at the point of sale and subsequently, the manufacturers’ rebate. The nonpartisan
Congressional Budget Office
(CBO) estimates that this will save the federal government a net $456 billion from 2022 to 2029. As the federal government reduces the amount of money it spends on drugs, it can also reduce the cost of premiums for beneficiaries. Accordingly,
CMS
predicts that beneficiaries will collectively save $117 billion, due to both lower premiums and lower cost-sharing.
The provision will invoke responses from pharmaceutical companies. The strict penalty of losing 65% of revenue would force pharmaceutical companies to negotiate, but over time, pharmaceutical companies may seek other methods to recoup their losses. For example, they may raise prices in other countries through rebates or complex pricing structures so that the AIM price increases. Furthermore, CBO estimates that this provision would lead to a loss of $ 0.5 trillion to $1 trillion in profit for pharmaceutical companies, and subsequently less pharmaceutical innovation by about 8 to 15 drugs over the next 10 years, although the White House and pharmaceutical lobbyists argue the number is
closer to 100
. However, the bill does allot additional funding to the NIH, which provided funding to
all 210 drugs
approved by the FDA from 2010 to 2016. Lastly, pharmaceutical companies may set enormously high prices for drugs that do not have an average international market price, knowing that they can still get 85% of the APM.
Inflation-Based Limit:
Policies proposing an inflation-based limit on drug prices require that pharmaceutical companies be penalized for price increases for Medicare Part B and/or D that have outpaced inflation. This provision mandates that drug companies must pay a rebate reflecting this increase directly to the government in an effort to address the rapid increase in drug prices and align price increases with the rate of inflation. The CBO estimates that the federal government would benefit from this provision because of the reduction in Medicare Part B and D costs. However, in order to counter the reduction in price, drug manufacturers may decrease the rebates paid to health plans, and thus, raise drug prices at the point of sale for beneficiaries. Because these rebates reduce premiums for beneficiaries and the overall cost of the drug, this could ultimately result in higher cost-sharing and higher premiums for beneficiaries.
|
|
Podcasts:
Further Reading:
|
|
|
|
|
|
|