When I think of sustainability, the first thing that comes to mind is partnership. Whether it is a marriage or a mission, a policy or a plan, making it sustainable requires collaboration. Rarely does major progress occur because someone acted alone.
In the space of our health care system, sustainability requires all stakeholders to play their part: It is the duty of our hospitals and their governing bodies to ensure that they meet community need. It is the responsibility of our elected officials to enact smart policies that move us toward a stable, safe, accessible and affordable health care system. And it is our regulator’s role to make sure hospitals have the financial wherewithal to treat their patients and serve their communities.
This kind of shared effort is no stranger to Vermont. When I got here almost six years ago, after working for a long time in conflict-driven Washington, D.C., I was quickly impressed by Vermont’s sense of community and common purpose. Even when there is serious disagreement, we handle it differently than in other places. The preference is for discord to be managed rather than magnified.
During the past two grueling years, Vermont’s version of this served our state so well. None of our mighty and envied response happened by accident. I saw it myself day after day, as hospital leaders worked side by side with government officials and other health care providers.
Vermont’s government agencies and our hospitals mobilized as a single unit, even when the unprecedented and unimaginable challenges came at us fast and furious. Instead of turf wars or disagreement on public health strategies (as happened in so many other states), Vermont kept doing the right thing, and doing it together.
Of course, this response is not an anomaly. It is an extension of decades of partnership to make health care work better for Vermonters. That partnership relies on a clear understanding of roles and a mutual respect for each other’s talent and expertise, which can then be harnessed in unison to meet the moment. Examples abound—from Dr. Dynasaur to Catamount Health to the All-Payer Model and now to our COVID response.
As our state leaders think about the future of health care and its sustainability, we must continue this proud tradition to ensure the strongest possible outcome. We all agree the system needs to be stable, which means protecting services in every corner of our state so that patients receive the care they need and deserve, and so our providers are assured of a system that values their contributions.
Hospitals and their heroic teams—which stepped up at every turn of the pandemic and contributed enormously to our effective response—must be protected and resourced, not accused and diminished.
There is plenty of space for disagreement and even tension as this important conversation takes shape. To best manage that, we must trust in each other to fulfill our respective responsibilities. If we do that—and always bring to the conversation our accountability and reason—we can produce real results for Vermonters.
|
|
Devon Green, VP of Government Relations
Last week, Vermont officially implemented the Nurse Licensure Compact. This licensure compact came after years of advocacy from VAHHS and other health care provider associations, as well as extensive work from the Office of Professional Regulation. It is all too easy to jump to the next emerging policy issue without taking a beat to properly acknowledge this type of accomplishment. I want to thank all those in the legislature and at the Office of Professional Regulation who made this happen!
Workforce: And, because the Nurse Licensure Compact will not solve all of our workforce problems, the House Health Care Committee heard testimony from Vermont’s higher education system on ways to support and expand nurse education. Current proposals include $1.5 million to expand K-12 education pipeline programs and Governor Scott’s FY ’23 budget proposal, adding $2 million to the nurse loan repayment program. The Vermont State Colleges system hopes to obtain $7 million to reduce its $7,000-per-semester tuition to more closely match the national average of $4,500 per semester. All of the representatives from higher education coalesced around increasing salaries for faculty and creating more opportunities for clinical placement.
Mental Health: The House Health Care and Senate Health and Welfare Committees heard from UVMMC mental health professionals about the need for more mental health services, including:
- Intensive out-patient programs to fill the current gap in care between in-patient services and community services
- Replicating the Psychiatric Urgent Care for Kids (PUCK) program throughout the state to lower emergency department utilization
- Increasing respite and mobile crisis capacity
Regulatory Flexibilities and Telehealth: This week, the Senate Health and Welfare Committee will take up H.654, which extends many current COVID regulatory flexibilities until next year. We appreciate their action on this as the current March 31st deadline looms large.
In telehealth news, the House Health Care Committee sent H.655, which creates a tiered approach to telehealth licensure, for a vote in the House. We really appreciate their quick action on this bill.
Blue Cross Blue Shield of Vermont testified that it currently reimburses audio-only mental health and substance use counseling services at 100 percent of the current in-person amount and all other audio health services at 75 percent the in-person amount. MVP Health Care will move to the same reimbursement model starting March 1. We appreciate Rep. Mari Cordes pointing out that audio-only health care services are not just phone calls, but actual health care services, and VAHHS supports 100 percent reimbursement of all audio-only services.
Health Care Reform: In its FY ’23 budget testimony, the Green Mountain Care Board urged the committee to appropriate $2-$5 million to study and implement global budgets for hospitals, as opposed to global budgets according to ACO-attributed lives and to optimize the health care system by reducing inefficiencies.
Alzheimer’s and Dementia: VAHHS advocated for coordinating and supporting current Alzheimer and dementia efforts as the Senate Health and Welfare Committee took up S.206. VAHHS asked for:
- One-stop website with community resources for patients, families and providers
- Continued support for current educational efforts to support diagnosis of Alzheimer’s Disease by primary care providers
- Support for the long-term care workforce to get patients to the right level of care and decompress capacity issues at hospitals
No Surprises Act: The House passed H.489, which allows the Department of Financial Regulation to enforce the provisions of the No Surprises Act federal legislation.
Prohibition of Firearms in Hospitals: The Senate passed a version of S.30, which prohibits firearms in hospitals and closes the “Charleston Loophole” with removal of a reference to 30 days. Due to this language tweak, the bill will now head back to the House before going to the governor’s desk.
|
|
Vermont joins national compact to make it easier for nurses to practice here |
Burlington Free Press
Faced with a nursing shortage deemed a "crisis" by state lawmakers, Vermont has joined a national compact with 38 other states to make it easier for nurses looking to work in Vermont to get a license.
Secretary of State Jim Condos said in a news release the Nurse Licensure Compact "provides mobility from the other 38 member states to enter into practice in Vermont without additional licensure requirements."
"Additionally, the (nursing compact) aligns with our goal to reduce barriers to licensure while ensuring public protection," Condos said. "Finally, the Compact enables rapid onboarding of vetted, competent nurses from other states into Vermont health care facilities at a time when the need has never been greater."
|
|
Hospitals waiting to feel relief from COVID-19 case decline |
NBC News
COVID-19 hospitalizations in Vermont are below 100 after a couple of weeks, and while the state of Vermont is noticing a decrease in cases overall, hospitals are still waiting to feel the relief.
"Our numbers in the ER in the hospital are still very very high. Last week was a very busy week for COVID," says Rick Hildebrant, Chief Medical Information Officer & Medical Director of Hospital Medicine at the Rutland Regional Medical Center.
More than 20% of Rutland Regional Medical Center’s inpatient capacity is taken up by COVID-19 patients.
"If someone has a stroke — and has a physical deficit because of that stroke — and is incidentally noted to have COVID, we can’t just send them to a nursing home or rehab center because they have isolation and restriction protocols," Hildebrant said.
|
|
Porter Hospital lab gets help from National Guard medics |
Addison Independent
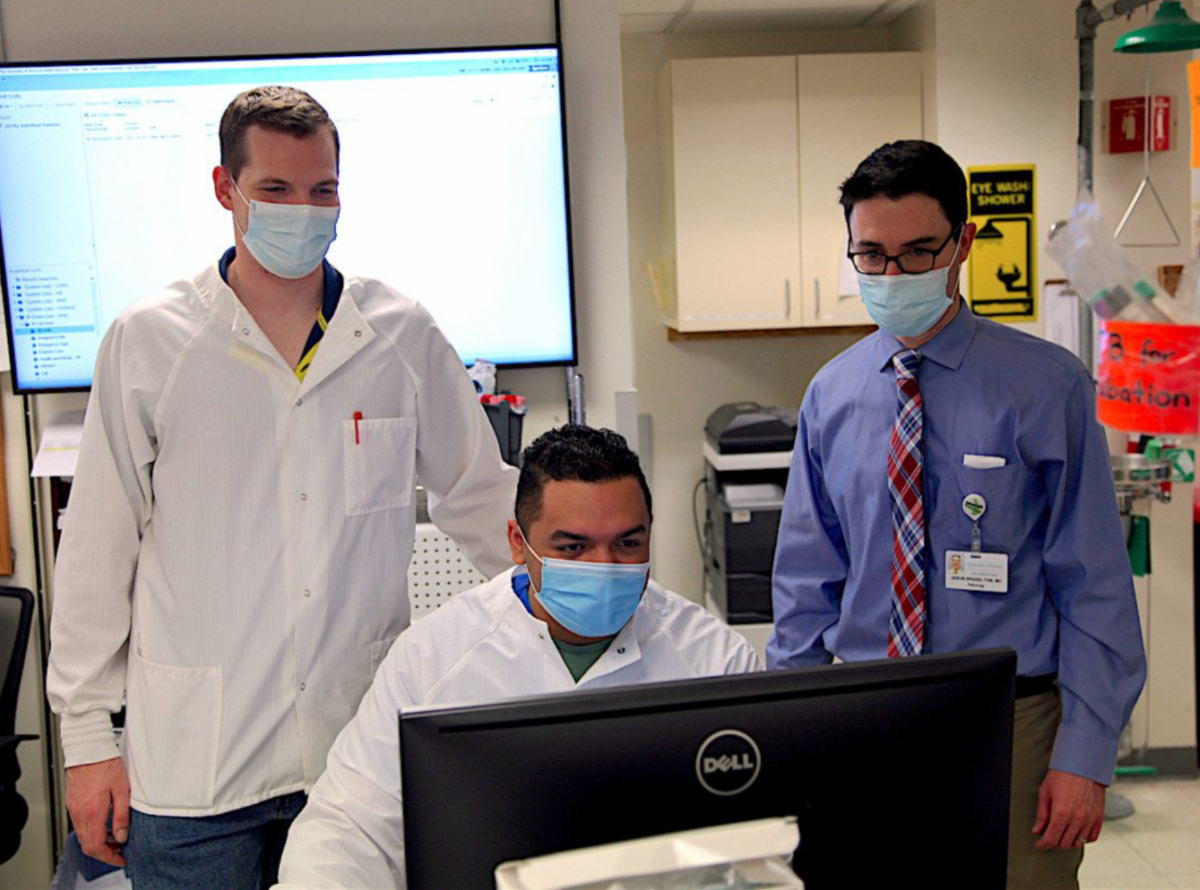
Two Vermont National Guard combat medics are helping Porter Medical Center get through a period of pandemic-related staffing shortages.
Pfc. Jeffery Perez and Sgt. William Glen began working at the Middlebury hospital’s laboratory this past Monday, Jan. 31, and will continue doing so through Feb. 18.
Last week, the Porter lab had to reduce its hours due to staffing shortages from both workforce pressures and absences related to COVID-19. The volume of COVID PCR tests at the hospital reached over 200 tests per day throughout much of January, in addition to blood draws and the other services the laboratory provides. Christopher Morris, Porter director of communications and engagement, noted that the surge in COVID-19 cases due to the omicron variant inflated the number of tests the lab had to conduct.
|
|
St. Albans hospital opens overflow wing |
VPR
Northwestern Medical Center in St. Albans had to open up a new wing to care for an unusually high number of patients.
Like other hospitals in the state, it hasn’t been able to transfer patients to nursing homes or speciality hospitals.
This backlog of patients comes on top of high demand in the emergency department and urgent care.
Northwestern Chief Medical Officer Dr. John Minadeo says every day is a challenge right now.
|
|
Lawmakers focus on state's mental health infrastructure |
Local 22
Wednesday marked mental health advocacy day in the Vermont legislature, and served as a reminder of the ongoing struggle to get people help when they need it.
In 2021, capacity pressures had caused logjams in Vermont’s mental health system, and children in a crisis were waiting days for treatment. Skip ahead a year, and those on the frontlines say things haven’t changed all that much.
“This Monday morning, there were 11 youth in the UVM emergency department for mental health needs, and their average length of stay at that point was 11.2 days,” said Haley McGowan, a child psychiatrist at the UVM Medical Center. McGowan said if you include kids waiting elsewhere in the hospital for a mental health placement, the average wait extends to 15 days. This appears to be the case in many hospitals.
|
|
How are Vermont’s hospitals faring? ‘We’re back from the edge’ as COVID numbers fall |
VPR
Hospitals across the state remain very busy, even as Vermont boasts one of the lowest COVID hospitalization rates in the country.
More surgical procedures are taking place, Vermonters are seeing shorter waits for care, and it’s generally easier to transfer patients from the hospital. “We’re not stretched as thin,” one health care provider summarized.
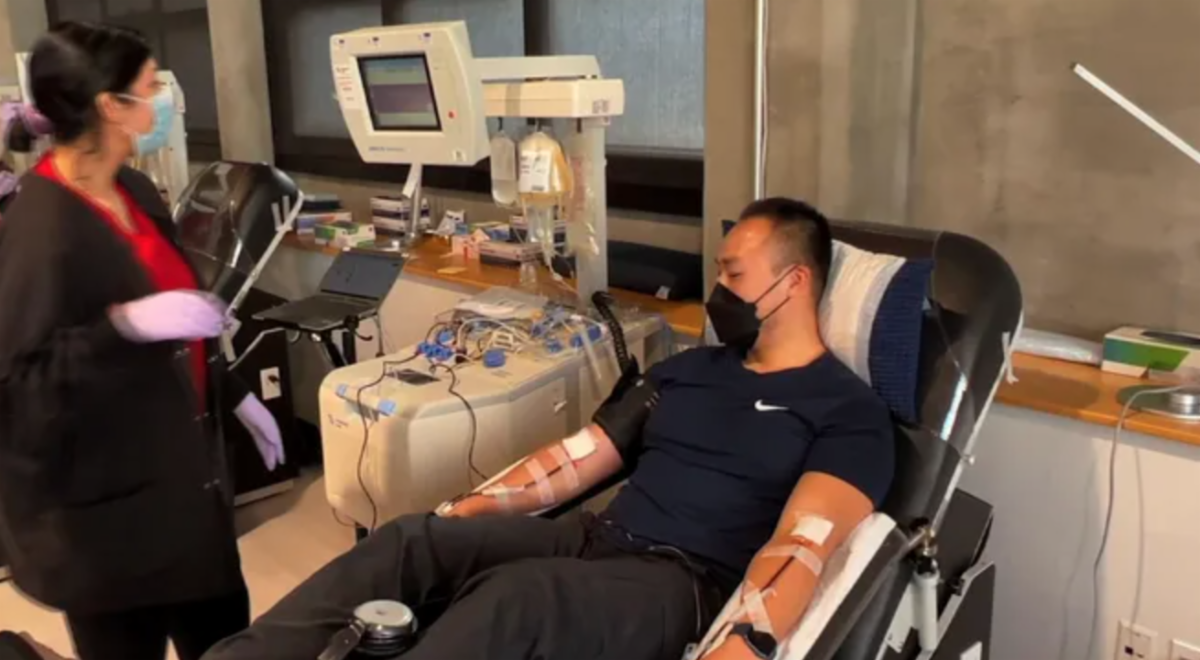
Still, hospitals are not functioning as normal. Nurses and paramedics contracted through the federal government and troops with Vermont’s National Guard continue to provide assistance. Blood supplies are at critical levels. And available hospital beds remain low.
|
|
Vt. lawmakers to consider funding hospital sustainability study |
WCAX
Can Vermont lawmakers keep cash strapped hospitals above water? A new proposal from state regulators aims to make rural health care financially sustainable.
In 2019, the Springfield hospital almost became a statistic -- one of more than 180 rural hospitals nationwide shuttered since 2005. After the facility filed for bankruptcy, policymakers in Montpelier sprang into action to make sure other rural hospitals stayed in the black.
From 2017 to 2019, six of Vermont’s 14 hospitals were in the red. Experts say the state’s aging population uses more resources and the pool of commercial insurance recipients is shrinking, driving up costs. The pandemic only made the situation worse.
|
|
Did Vermont hospitals get ‘overwhelmed’ during Omicron surge? |
VTDigger
As Vermont’s Covid-19 cases and hospitalizations continued to trend down, Health Commissioner Mark Levine celebrated the state’s resilient health care system during the governor’s weekly press conference Tuesday.
“At no point during the Omicron surge, even when our hospitalizations were in the 120 range per day (of patients with Covid) and the number of ICU beds and use were in the high 20s, did the state’s health care system capacity become overwhelmed,” he said.
|
|
|
|
|
|
|