|
Back in the days when beer was tuppence a pint and you could get drunk for a shilling…
… a pair of step ladders, dust-sheets, a pot of white paint and a nine inch brush, parked in the middle of an empty hospital ward, was not an unfamiliar sight.
The only way hospital bosses, could balance their budgets was to slow down elective surgery.
The problem was…the local Community Health Council would have to be consulted and they would never agree to ward closures.
The Councils comprised local councillors, voluntary sector, community leaders and the public.
They were tough...
... knew the hospitals, knew the managers, knew the patients, knew the public, and…
… they also knew they couldn’t stop hospitals closing wards for redecoration!
Both sides knew what was happening and they coexisted in the subterfuge. They were formidable, committed people.
In 2001 Alan Milburn (yes, him again), abolished them.
Various iterations of public engagement followed, nothing really worked. In 2013, Healthwatch emerged.
Now Milburn is back, running the NHS again, guess what… Healthwatch is being abolished.
Without a statutory body empowered to challenge local decisions, NHS organisations will face less public scrutiny.
That risks decisions being made more for organisational convenience or financial targets than for patient need.
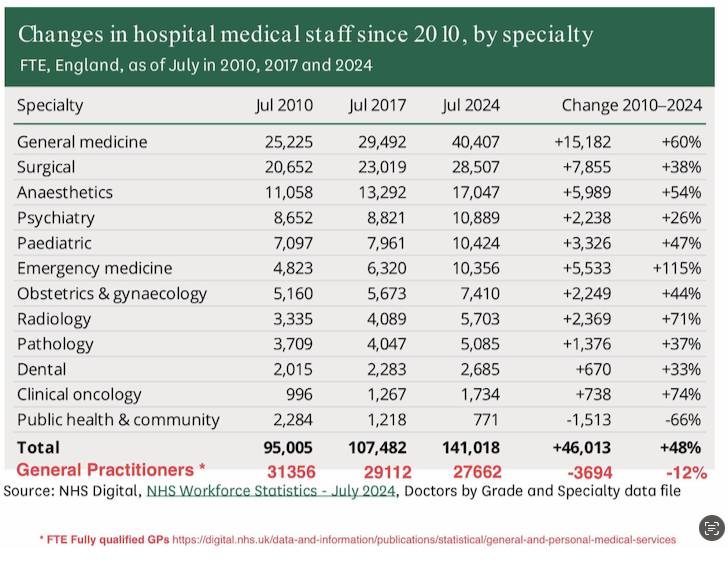
We saw it last week, with the league tables. Made entirely useless for the public by the weighting given to finance... obscuring all other issues.
CHCs had legal rights of entry into hospitals and the ability to hold boards to account.
Healthwatch, though weaker, still gathered intelligence and evidence on patient experience.
The loss of that leaves patients with fewer routes to escalate concerns.
Instead of a single recognisable voice, feedback risks being scattered across charities, campaign groups and social media outrage...
... which makes it easier for HMG and NHSE to dismiss dissent as, anecdotal.
A publicly funded service needs visible mechanisms for the public to be heard.
Without that, trust declines and the sense of the NHS being ‘ours' diminishes.
Milburn is a managerialist with a market-facing view of the NHS. His moves often tilt towards making the service easier to reshape, centralise, or open to new providers.
It seems to me he thinks public-voice-structures slow reform, gum up decision-making, or get ‘captured’ by activists. I think I recall that was his criticism of CHCs all those years ago.
Removing an organised public voice makes it easier for ministers to push through difficult reorganisations, cuts, or market reforms without a statutory check.
I’ve always thought he tended to favour patient choice and consumerism...
... the concept of the individual voting with their feet...
... as more powerful than collective structures like CHCs.
The closure of Healthwatch reflects that same preference…
... let individuals speak through choice of provider, surveys and digital feedback, not through a statutory body.
The loss of Healthwatch continues a long trajectory away from collective, statutory patient-power, towards individualised, consumer-style feedback.
The risk is… it hollows out democratic legitimacy in a service the public fund and cherish, but…
… choice is illusory.
Most patients want timely, safe, decent care at their nearest hospital. They don’t want to shop around… particularly if they are unwell.
For many services, there is only one local option, so the competitive dynamic Milburn envisaged, never really materialises.
Emergency care is not elective. You don’t choose your A&E when you’re in an ambulance.
Even for planned surgery, choice is narrowed by clinical advice, transport links, post-procedure follow-up and family support.
Competition hasn’t delivered. Studies of NHS market-style reforms show negligible impact on quality and the administrative burden often outweigh benefits.
Competition always increases costs, by duplicating back-office functions and incentivising ‘gaming’ of performance metrics.
What raises quality is usually collaboration, multidisciplinary teams, integrated care pathways, sharing expertise. Competition pulls in the opposite direction, encouraging silos and duplication.
Patients value voice over choice.
What people consistently say they want is influence… the ability to have their concerns heard, their local services shaped by local needs and their complaints acted upon.
CHCs, however imperfect, gave that. Healthwatch is an echo of it and now dumped.
Milburn dismantled CHCs in the name of modernisation, pushed choice as the public voice, but the reality is...
... the public never wanted to behave as consumers.
They wanted to be citizens with a voice...
... not customers with a voucher.
|