|
VOR's Weekly News Update
VOR is a national non-profit organization
run by families of people with I/DD and autism
for families of people with I/DD and autism.
| |
|
Please join us on Capitol Hill
May 12-14, 2025
VOR's Annual Legislative Initiative
Washington, D.C.
| |
|
We will meet in D.C. on May 12th - 14th
for meetings with
Congressional Staff and Federal Agencies
to discuss issues of critical importance to
individuals with severe or profound I/DD and autism
and their families.
This year's topics are expected to include:
Preventing Cuts to Medicaid
and
Rebuilding and Supporting our DSP Workforce
This event is open to all members of VOR
Please register early, to reserve your spot
Registration is free until February 1, 2025
So please register now!
To register for the Legislative Initiative,
Please Click Here
| |
Sponsorship Opportunities
This is a critical time for our families.
The actions taken by Congress and the Administration
in the next few months could impact the lives of
hundreds of thousands of people with I/DD and autism in the years to come.
Please help us help.
Diamond - $ 5,000
Platinum - $ 2,500
Gold - $1,000
Silver - $ 500
Bronze - $ 250
Advocacy Hero - $ 100
Friends & Families - (Other amounts)
| |
Any and all gifts are welcome | |
It's All About The Medicaid: | |
|
Medicaid, Medicaid, Medicaid.
People don't seem to know whether to be tired of discussing it or determined to keep fighting for it.
At VOR. we are determined to fight for it. And we hope that our members will join us.
While our two political parties have taken sides on this issue, this is NOT a political issue for VOR's families. It is a matter of survival, for Medicaid is the foundation upon which all other I/DD, autism, mental health, and aging issues stand. We cannot afford to lose it.
It's also very much a moral issue. Are we a country that cares about our most vulnerable citizens? Or is money the only thing that matters? At VOR, we care about our people.
So we ask that you try to see past the political rhetoric, and look at the facts of Medicaid, and do whatever is in your power to protect it, for all of our families.
Hang in there. We only have a few more weeks to determine whether we can preserve this vital program, or watch it crumble into the dust of a different era.
| |
Fact Sheet: Medicaid
American Hospital Association, February, 2025
The Issue
The Medicaid program is the largest single source of health care coverage in the United States, covering nearly half of all children, over 40% of births (including nearly 50% of births in rural communities), many low-income elderly and disabled individuals, and working adults in low-wage jobs that do not offer affordable coverage. Congress is currently considering policy options that could collectively reduce federal spending for the Medicaid program by trillions of dollars over the next 10 years. These options include proposals to directly reduce federal spending on the program and limit states’ ability to generate funding for the state share of the costs.
AHA Take
Even a small portion of the proposed reductions could have wide-ranging negative consequences for the health and well-being of both Medicaid enrollees and the broader health care system. AHA urges Congress to reject reductions to the Medicaid program that would not only strip access to health care from some of the most vulnerable populations but also destabilize hospitals and health systems, leading to a loss of services that would impact patients and communities nationwide.
Why?
- Medicaid provides critical health coverage to a wide variety of people in every community across the nation. This coverage helps ensure patients can receive the medical services needed to live healthier and more productive lives.
- Medicaid covers over 40% of births in the U.S., including nearly 50% of births in rural communities. It is also a vital source of prenatal and postpartum care for women across the country.
- State Medicaid programs pay hospitals less than the cost hospitals incur to provide care to Medicaid patients. In 2023, the difference between Medicaid payments and costs, known as “Medicaid shortfall,” was $27.5 billion.
-
Medicaid is an important source of support for the health care system. The impact of cuts to Medicaid would not be limited to just Medicaid beneficiaries. It would stress the availability of health care services for everyone. Today, hospitals that serve disproportionately high rates of Medicaid and other public-payer patients routinely operate with negative margins and are often forced to terminate service lines or close entirely. Reductions in federal support for Medicaid would exacerbate these pressures, which could strip essential health care services for an entire community.
- Medicaid is one of the most cost-efficient forms of coverage. It has lower total and per capita costs than all other major health programs, including Medicare and private health insurance.
- Most of the spending on Medicaid is for disabled and elderly individuals. States could not absorb the magnitude of the proposed cuts by solely reducing enrollment or services for working-age adults — the disabled and elderly populations would also be negatively impacted.
Continued
| |
House GOP Makes Official Its Plan For Devastating Cuts To Medicaid
By Nicole Lafond, Talking Points Memo, February 12, 2025
In announcing their intentions to move forward with a mammoth one bill budget plan that will supposedly sweep up key elements of Donald Trump’s fiscal agenda, enact tax cuts and raise the debt ceiling, House Republicans have placed themselves on a collision course with not just members of their own conference but also Senate Republicans.
But one thing is clear now that has been clear for months: Medicaid, the program that covers health care costs for low-income Americans, is, by design, the main target of the House GOP’s federal spending cuts proposal.
Here’s a breakdown of the key elements of the budget blueprint, which the House Budget Committee released the text of Wednesday:
- House Republicans want to enact $4.5 trillion worth of tax cuts over the course of the next decade, some of that will include extending Trump’s 2017 tax cuts that provided the most benefits to wealthy Americans.
- They propose $2 trillion in federal spending cuts.
- Those spending cuts would offset the cost of the tax cuts, but only partially, meaning the entire proposal would actually end up adding trillions to the national deficit, roughly $3 trillion over 10 years, by the New York Times’ calculation.
- That coupled with plans to raise the debt limit by $4 trillion has fiscal hawks in the House howling, Politico reported. Hardliners in the House Freedom Caucus are reportedly pressing for at least another $500 billion in spending cuts to be outlined in the proposal, plus they want to see work requirements (another GOP word for spending cuts) for Medicaid, food aid benefits and at least one other social safety net program made explicit in the resolution.
- It is not entirely clear where the $2 trillion in cuts will come from, rather the House Budget Committee is proposing that various committees find enough savings to hit fixed spending reduction targets.
So while it is not explicitly stated in the House Budget Committee’s document, Medicaid and Supplemental Nutrition Assistance Programs are the programs most directly in the crosshairs. Here’s why: The document charges the House Energy and Commerce Committee with finding $880 billion in ten-year savings, more than half of the total cuts outlined in the proposal. It also directs the House Committee on Agriculture to identify another $230 billion in cuts. The Energy and Commerce Committee oversees Medicaid spending and the Ag panel has jurisdiction over SNAP and other nutritional programs.
While House Speaker Mike Johnson (R-LA) has pushed work requirement rhetoric in recent days when pressed on the nature of potential impending cuts to Medicaid and other social safety net programs, the magnitude of the spending reductions being proposed means cuts to Medicaid will have to extend far beyond Republicans simply imposing work requirements. That language has become a rhetorical catchall for Republicans for months as they sidestep engaging seriously on the political ramifications of cutting programs for low-income Americans to extend tax cuts for the wealthy.
Continued
| |
Republicans May Find It Harder to Cut Medicaid Than They Think
The program’s surprising superpower? It’s popular.
By Joanne Kenen, Politico, February 13, 2025
Republicans may have just gotten an alarming glimpse of the future.
Amid the chaos of President Donald Trump’s now-rescinded domestic funding freeze, Medicaid portals across the country went offline, which meant states couldn’t get their Medicaid dollars. It was something the administration said was never supposed to happen and which provoked public outrage and a bipartisan outcry.
Now Republicans are considering whether and how to target Medicaid as part of their effort to defray the cost of massive tax cuts, the centerpiece of Trump’s legislative agenda. With full GOP control of Washington, the question at the start of the year seemed to be not whether Medicaid would be cut but by how much. Republicans passed around proposals just last month that would slash hundreds of billions of dollars from Medicaid and radically transform the program. Yet this week, Speaker Mike Johnson suggested the deepest cuts might not be in the offing. GOP lawmakers are still haggling over their budget blueprints amid a fierce debate between hard-liners and relative moderates over spending cuts.
As the blowback over the portals foreshadowed, going after Medicaid will be harder than it looks. That’s because the program has evolved and expanded significantly over the years — and its constituency has expanded along with it. Some 80 million people now get health care from Medicaid, including many working-class voters in the president’s base.
During the 2024 campaign, Trump frequently reassured jittery Americans that he wouldn’t lay a finger on their Social Security or Medicare. Medicaid didn’t get the same protective promises, though Trump last month remarked he’d “love and cherish” the program. In recent days, Trump and his aides have said privately that they are worried steep Medicaid cuts would be politically radioactive, POLITICO reported.
Patrick T. Brown, a fellow at the conservative Ethics and Public Policy Center, who has pushed the GOP to embrace more pro-family policies, said the party faced internal tensions. Traditional GOP budget hawks see the current moment, he said, “as an excuse to do what they wanted to do all along, which is slash social spending and, ideally, return to the days before the Affordable Care Act.”
But, he noted, a political realignment is taking place with the GOP increasingly appealing to voters who rely on government programs: “You can say President Trump was elected on a mandate. But the mandate was not ‘Let’s slash health care from working-class Americans.’”
Polling data backs him up. Public opinion surveys detect growing popularity for Medicaid across the political spectrum. And in the seven states that have had ballot initiatives on Medicaid expansion, it’s won with striking margins. That includes deep-red places like Idaho and Utah.
A 2024 poll conducted by the nonprofit health research organization KFF found that 71 percent of voters wanted Medicaid to remain more or less the way it is today, including more than half of Republicans. And 77 percent of people surveyed recently viewed the program favorably, including 63 percent of GOP respondents.
Such broad support may not be surprising considering how many people have a direct connection to the program. Roughly two-thirds of adults in the United States say they or a family member or close friend have relied on Medicaid.
Republicans on the House Budget Committee considered a plan Thursday that could lead to Medicaid cuts as deep as $880 billion over the next 10 years. The proposal faces numerous hurdles, but it’s a key part of the reconciliation process, which would allow legislation to pass with just a simple majority in the Senate and can’t be filibustered by Democrats.
So what might Republicans try to do to Medicaid?
Some conservatives are pushing to establish per capita caps, which means Medicaid would no longer be an open-ended entitlement program. States would get a fixed amount each year, along with more flexibility on how to spend it, but growth of the program would probably not keep up with people’s needs. The idea of a cap or similar block grant has been around since the Reagan administration. But it’s always been a step too far — and that’s probably true this time around as well.
One more likely move is to impose work requirements on those enrolled in Medicaid in some or all states, either through legislation or federal waivers. Millions of Medicaid recipients already work — and it’s unclear how well those who are disabled would be shielded from requirements. In addition, documenting work is extremely cumbersome. That’s what cost thousands of working people on Medicaid their coverage in Arkansas, before the requirements were halted. Courts have been skeptical of work requirements in the past, as the Medicaid statute is about health, not employment. But Trump moved the courts to the right in his first presidency.
States or the federal government could also tweak rules and procedures in ways that make it administratively harder for people to enroll in Medicaid or stay enrolled. One Republican mantra is the need to root out “waste and abuse” — but how lawmakers would define that is far from clear. The Trump administration could also limit or stop states from using Medicaid dollars to address needs like housing or food insecurity, so-called social determinants that drive poor health.
Neither Trump’s newly confirmed HHS secretary, Robert F. Kennedy Jr., nor his pick to oversee the Centers for Medicare and Medicaid Services, Mehmet Oz, have put forth their views on what, if any, of these scenarios they favor. Kennedy answered questions about Medicare and Medicaid vaguely and often inaccurately at his confirmation hearings. Oz’s hearings have not taken place.
Tom Miller of the center-right American Enterprise Institute is a longtime critic of what he calls Medicaid’s “bloat.” But he said he’d rather see a thoughtful, policy-driven overhaul that focused on people who really need government help, rather than the cost-cutting initiative seemingly taking place.
Read the full article here
| |
The Biggest Health Policy Decisions Now Facing the Trump Administration
By Drew Altman, KFF, February 14, 2025
Decisions about two things—paying for tax cuts, and whether President Trump wants another big fight about health care—more than any other factors, will drive the biggest health policy decisions in the early days of the Trump administration.
The first big decision is the one Republicans will make about paying for their $5 trillion tax cut (coincidentally about the same amount as we spend on health care each year). After plans were floated in the House for Medicaid cuts totaling an astronomical $2.3 trillion, Republicans appear to be circling around plans for Medicaid cuts in the neighborhood of almost $900 billion over 10 years. No number or program cut is cast in stone yet and the health policy environment is fluid and unpredictable as a result. But tax policy, coupled with a general desire to cut back the role of the federal government, is the major factor driving health policy.
That leads to the second big decision. Does President Trump want another big health care debate? Any of the big Medicaid proposals floated so far—a per capita cap, drastic cuts in federal Medicaid expansion matching rates effectively killing the expansion in 40 states and DC, or significant cuts in the regular Medicaid matching rate, and Medicaid work requirements—will bring a divisive debate. With margins tight in the House, the President may not want to run the risk of another defeat on a big health care package, having suffered a dramatic defeat on the Affordable Care Act (ACA) repeal in his first term. Instead, he may decide to keep health care, with its incendiary politics, out of the picture and avoid handing Democrats a hammer to use to drive down his popularity and wield in the midterms. Conservative Republicans in the House have a clear policy agenda to reduce federal health spending and the federal role in health. President Trump is more transactional and focused on his popularity, which is up, from 47 to 53 percent, momentum he will be careful not to squander.
It’s possible, if not likely, that Republicans in the House and President Trump will try to find a goldilocks solution to the tension between their goals: cut enough in federal Medicaid spending to help pay for tax cuts and satisfy conservatives who want to reduce federal spending, but not so much as to generate a controversial debate that endangers Trump’s ratings. That will not be easy. So far, the Trump administration’s actions in health have focused mainly on populations and programs without much political power, leaving hospitals, doctors, the nursing home industry, the managed care industry and state budgets generally untouched. Significant cuts to Medicaid will change that equation. Medicaid itself touches a broad swath of the population, with around 50% of the American people reporting that they or a family member have been covered by the program at some time. More than half of Medicaid spending goes for people who qualify for the program based on disability or age, many of whom use long-term care, including in nursing homes, which generally have powerful lobbies at the state level. Half of all Medicaid spending flows to the managed care industry, which is dominated by big insurance companies. Republican governors often turn on policy ideas that sound good until they morph into cuts in their federal funding that threaten state budgets and a governor’s popularity. There is no significant cut in Medicaid spending that is easy or simple to pull off, and certainly not one totaling almost $900 billion dollars over 10 years.
Continued
| |
New Congressional Attempt to Cut Medicaid Through Budget Reconciliation
By Julie Carter, Medicare Rights Center, February 13, 2025
This week, the House of Representatives is trying to lay the groundwork for rushed and drastic cuts to Medicaid and other supportive programs. These cuts would take health care away from people who need it most, including older adults, people with disabilities, and children who get their health insurance from Medicaid to support them in their homes and communities. No one with Medicaid is safe from these cuts.
Outline of Budget Reconciliation Process
The budget reconciliation process does not follow normal rules in the Senate and would therefore allow Congress to rush through these cuts. Essentially, it is a mechanism that allows the Senate to bypass the typical 60 vote filibuster threshold and pass certain tax and spending changes with just 51 votes. It does not apply in the House where, like other bills, a majority would continue to be needed for passage. There are complicated parliamentary standards that reconciliation bills must meet to get this privileged treatment in the Senate, but bills that comply can be used to make consequential changes, including to key health care programs like Medicare, Medicaid, and the Affordable Care Act. Most recently, lawmakers used reconciliation to pass the Inflation Reduction Act under President Biden and tax cuts under President Trump.
Essentially, it is a mechanism that allows the Senate to bypass the typical 60 vote filibuster threshold and pass certain tax and spending changes with just 51 votes.
The process starts with the budget committees of the House and Senate writing budget resolutions that call for reconciliation. Those instructions tell certain other committees how much they are required to spend or save on programs under their jurisdiction. Each Budget Committee and chamber must vote on whether to accept the reconciliation instructions. Once approved, the committees begin writing bills that meet their targets. Those drafts are then packaged together and any differences between the House and Senate versions must be worked out prior to final passage.
Competing Instructions in the House and the Senate
This year, the House and the Senate are taking different approaches to budget reconciliation, with the House trying to do a single, massive bill and the Senate pursuing a two-bill strategy. Work in both chambers is underway.
The House is marking up its draft budget resolution today, February 13. As proposed, it would require deep cuts to programs that support health, food, and safety to fund tax cuts and hikes to the defense budget. It specifically directs the Energy and Commerce Committee to reduce spending by at least $880 billion. Medicaid is the largest program this committee oversees and the only plausible source for these potential cuts. Importantly, this target number is a floor and not a ceiling; lawmakers could cut even more as the process advances.
Medicaid is… the only plausible source for these potential cuts.
After the budget resolution passes out of committee, it will move to the full House for consideration. Republican leaders are targeting the week of February 24 for that vote.
The Senate instructions for their first bill are farther along; the budget resolution passed out of the Budget Committee yesterday along party lines. It prioritizes military and security programs, directing those committees to increase spending by $342 billion. It does not fully pay for this hike, but it does direct the Senate Finance Committee to cut at least $1 billion, most of which would likely come from Medicaid. As with the House instructions to the Energy and Commerce committee, this number could also grow over time. And a two-bill strategy would give the Senate another opportunity this year to pursue harmful Medicaid cuts.
The full Senate may consider its budget resolution the week of February 18.
Risks to Medicaid
There are a number of ways Republican lawmakers could try to cut Medicaid in a reconciliation bill, all of them harmful. The House Budget Committee previously released a list of potential policies, ranging from eligibility changes to funding rollbacks.
One option is to limit the federal help states receive. Currently, states work with the federal government to fund Medicaid and receive a fixed percentage (the FMAP) every year. Slashing these percentages would save federal dollars, while forcing states to either cut their Medicaid programs or pay for them solely from state funds. Since most states would likely be unable to maintain current coverage and services without appropriate federal assistance, this could lead to widespread cuts and millions of older adults and people with disabilities losing access to needed care and supports.
Similarly, some lawmakers have proposed moving Medicaid to a capped program. This too would reduce the federal government’s role and financial support. There are a several approaches a restructuring could take, but under the recently floated policy, states would receive a fixed amount of federal Medicaid funding on a per-beneficiary basis, “based on a preset formula, which [would] not increase based on actual costs. States exceeding the ‘cap’ for enrollees would thus need to find other revenues to maintain spending levels or explore innovative ways to reduce excessive costs.”
To maximize federal savings Medicaid funding caps are typically not intended or designed to keep pace with expected health care cost growth, creating funding shortfalls that grow larger over time. As these deficits mount, states would have little choice but to curtail costs on an ever-growing scale, eventually cutting critical lifelines for older adults, people with disabilities, and their families.
Older adults and people with disabilities would likely bear the brunt of any Medicaid cuts, as their health care costs comprise more than half of all Medicaid spending.
Older adults and people with disabilities would likely bear the brunt of any Medicaid cuts, as their health care costs comprise more than half of all Medicaid spending. According to a recent KFF fact sheet, nearly 1 in 4 Medicaid enrollees are eligible for the program because they are ages 65 and older or have a disability, and they have higher per-enrollee costs “than other enrollees due to more complex health care needs, higher rates of chronic conditions and being more likely to utilize long-term care.”
Medicaid is the primary payor for long-term services and supports for people who need home and community-based services and nursing home care, and it also plays a vital role in helping support family caregivers.
Increasing red tape is also in play, with the potential to require enrollees to jump through administrative hoops in the form of work requirements or more frequent redetermination that both cause people to lose coverage while still being eligible. Paradoxically, work requirements and other administrative barriers are extremely expensive for states to set up and maintain. They have also not been shown to increase employment, only to decrease coverage.
[Medicaid work requirements] have also not been shown to increase employment, only to decrease coverage. .
Take Action to Protect Medicaid
As Congress contemplates next steps on budget reconciliation, we need to send a clear message: Don’t cut Medicaid! Join Medicare Rights and advocates across the country today.
- Use this call-in line (provided by SEIU) to reach your lawmakers: 866-426-2631.
- Tell them to oppose any Medicaid cuts. Whether it’s work requirements, eligibility changes, or reduced funding, a cut is a cut.
- A cut to Medicaid is a cut to Medicare. The programs work together to provide the services and supports people need.
- And the outcome from any cut is the same: older adults, people with disabilities, and their caregivers would lose access to needed health and long-term care.
- Medicaid is a lifeline for over 7 million older adults and 12 million people with Medicare. Slashing the program would cause serious and lasting harm.
- Be sure to personalize your message! View this map to learn what percentage of people in your Congressional district rely on Medicaid and share that number with your lawmakers.
Read the full article here
| |
|
Many VOR members are familiar with one of the two authors of the article below. Alison Barkoff is the past Deputy Administrator of the ACL, and a fierce advocatee for one-size-fits-all policies that have harmed the ICF system over the years. Nonetheless, she and her colleague provide a concise picture of the state of Medicaid in the reconciliation process. So please don't shoot the messenger just now.
What Lies Ahead For Medicaid In Budget Reconciliation?
By Sara Rosenbaum and Alison Barkoff. Health Affairs, February 11, 2025
President Trump recently stated, “We will love and cherish” Medicaid, promising that budget cutting would be limited to finding waste and abuse. But that sentiment is not likely to prevail as Congress moves forward with massive budget cutting efforts, to be carried out in either one or two phases. (The strategy is not yet clear.). Indeed, given the proposals that have surfaced, it is evident that tens of millions of people face a high risk of losing Medicaid coverage and services, either through significant cuts to federal funding or imposition of a work mandate with complex reporting requirements as a condition of eligibility, or a combination of the two.
Should Congress pursue a wide range of possible budget-cutting strategies, all Medicaid populations, from the youngest infants to the most vulnerable older adults, inevitably will feel the effects. Moreover, the safety net health care providers that disproportionately serve the poorest and highest-need patients, and indeed the health care system as a whole, will be at risk. The changes under consideration, if enacted, would shake Medicaid’s very structural foundations and imperil its future as the nation’s largest public health insurer.
Some have claimed that older adults, those with disabilities, pregnant women, and children will all be protected. There have even been claims (especially in the case of cuts to working age adults) that these changes are necessary to protect these populations. Obviously these claims are not simply wrong but completely disingenuous. There is simply no way to protect any beneficiary from the impact of far-reaching Medicaid spending reductions. Medicaid is perhaps the nation’s most complex federal health care program, and each element of the program is inextricably connected to the other. Taking unprecedented sums out of Medicaid would hurt everyone. Period.
Public health experts have raised alarms over these developments. Equally breathtaking for a health insurance program that currently insures over 80 million children and adults and represents nearly 20 percent of all national health expenditures, proponents of deep reductions have narrowly cast their efforts as “cost savings” in an attempt to deflect public attention from the real plan—to fundamentally shift Medicaid policy to advance an agenda put forth by people who, for philosophical reasons, have long trained their sights on unraveling Medicaid. Indeed, massive Medicaid restructuring was a principal element of Project 2025, the policy blueprint that fueled President Trump’s campaign.
The Budget Reconciliation Process
Senate Budget Committee Chairman Lindsay Graham has now released the text of his committee’s draft FY 2025 budget resolution , which is expected to be the first of two such resolutions in the Senate. The House is still struggling to assemble a single gigantic resolution rather than moving two separate bills. Regardless of the process used, both the House and Senate are expected to instruct their respective authorizing committees (Energy and Commerce in the House, Finance in the Senate) to significantly cut Medicaid spending. Whatever the resolutions’ final numbers, they are merely a starting point or floor; based on all reports, spending reductions are expected to go far deeper.
The process of altering actual spending, including spending on “mandatory” programs like Medicaid, to reach the target number is known as the budget reconciliation process. A key check on budget reconciliation in the Senate is known as the Byrd Rule, which is designed to keep the fast-track legislative process used for reconciliation (requiring only a simple majority in the Senate rather than a filibuster-proof 60-vote threshold) focused on raising revenue or cutting outlays. As a result, the Rule, in effect since 1985, offers some safeguards against legislative changes that may have an indirect outlay effect but nonetheless are so speculative as to not be able to generate predictable, measurable savings. For example, simply reauthorizing a program is considered extraneous because without actual funding, reauthorization has no budgetary impact.
Importantly, changes considered tangential to the task of saving money—for example changes that may involve a policy whose budgetary effects are speculative at best—would be considered extraneous. But these are calls for the Senate Parliamentarian and the Congressional Budget Office and it is impossible to know what ultimately could qualify for inclusion. (This deliberation process is known as the “Byrd Bath.” History shows crucial behind-the-scenes battles over what is in and what is out).
Thus, any discussion of potential Medicaid cuts will be inevitably influenced by the budget process itself, which is designed to focus on achieving measurable spending reductions that at least meet the budget targets. The Medicaid target floors remain fluid at this point; nor do we know how CBO will score a specific proposal or which proposals might be considered extraneous in the Senate. Nonetheless, given the white-hot focus on the nation’s largest means-tested entitlement program—further intensified by the OMB’s federal spending stoppage that initially included closing off the federal Medicaid payment system on which states, providers, and beneficiaries depend—it is possible to describe the preliminary changes on the table and t]heir implications.
Importantly, in any effort to cut Medicaid spending, negotiations are really a four-sided table, including the House, the Senate, the White House, and the states. States not only bear a significant proportion of total Medicaid expenditures but also face major challenges in generating that share; they depend deeply on Medicaid as the single most important federal funding source and a bedrock within their economies.
Fundamentally Altering The Federal/State Financial Relationship
For sixty years, states have participated in Medicaid based on certain basic promises about the federal funding to which they are entitled. Decisions about program scope and size are inextricably tied to states’ near- and long-term projections about the funding they will receive. They have been able to do this because for over six decades the contours of Medicaid funding have remained fundamentally stable, with periodic temporary adjustments to deal with exceptional costs such as the federal spending increase during the Covid pandemic. These rules of the game are the bedrock on which Medicaid rests.
A Three-Part Deal: An Open-Ended Federal Payment Share
As part of Medicaid’s 1965 enactment, the federal and state governments entered into a basic three-part deal. First, states would be given considerable latitude to determine the size and scope of their programs within certain federal parameters, the most notable being coverage of certain populations for a wide range of medical assistance services. Once a state chose to cover a population, those beneficiaries would be entitled to covered services. States, in turn, would be entitled to payment of the federal share for services provided, with open-ended financing available to enable states to meet the cost of medically necessary care.
This structure—federal contributions to state expenditures on an open-ended financing basis—represents the crucial promise on which Medicaid was founded. Given who depends on Medicaid – infants, children, pregnant women, the poorest working-age adults, children and adults with disabilities, and a large aging population—the promise of open-ended financing is crucial.
A Three-Part Deal: A Sliding Federal Share Based On State Income Levels
Second, depending on population income levels, participating states are entitled to federal reimbursement of between 50 and 83 percent of their medical assistance expenditures furnished under its approved state plan, as well as at least 50 percent of program administration costs. States are also entitled to certain payment enhancements, which may be temporary or permanent. For example, during the COVID pandemic Congress temporarily increased federal Medicaid funding levels to help states meet the cost of continuous eligibility for coverage. The Affordable Care Act Medicaid expansion was predicated on a highly enhanced permanent federal financing level of 90 percent and is basic to states’ participation decisions.
A Three-Part Deal: An Obligation To Spend State Funds
Third, a state would be expected to spend its own funds to partially fund its Medicaid program—at least 40 percent of total non-federal expenditures, with the remainder coming from local governmental contributions (e.g., county expenditures for publicly supported hospitals and clinics; health care revenues generated by local taxing authorities). To meet their expenditure requirements, virtually all states today employ, among other tools, their authority to impose broad based provider taxes. Such taxes can make up a considerable proportion of total state expenditures, with the rest coming from general revenue sources.
Republican Ideas For Altering The Federal-State Deal:
The most obvious way to cut hundreds of billions, if not trillions, of dollars in Medicaid outlays is to make fundamental changes to this longstanding deal. Below are concepts that Republicans in Congress have already put on the table for consideration.
Capping Federal Spending
Congress could impose either block grants or per capita caps (spending limits per person) that restrict total federal contributions to state programs. Both of these proposals would renege on the time-honored promise of how the federal government funds Medicaid and would translate to significant cuts in Medicaid funding over time. Per capita caps, which have received more attention, have been projected by the Congressional Budget Office to cut more than $900 billion over a decade, depending on how the cap is set.
Budget experts assume that per capita caps would result in deep federal payment reductions below what states otherwise would be entitled to receive. Per capita caps also would shift considerable costs to states, thereby necessitating either new state revenues to fill the hole or, more likely, major reductions in coverage of costlier optional populations and services, especially low-income seniors and people with disabilities; institutional and community-based long term services and supports for children and adults (including older adults) with significant disabilities would be on the chopping block. Per capita caps would particularly penalize states that attempt to more comprehensively support their sickest and highest-need populations, states whose demographics skew older and high need (think Rust Belt states), and states with the highest health care costs.
Read the full article here
| |
A Brief Moment of Clarity: | |
“Nothing About Us Without Us” Leaves Voices Out
By Doreen Samuelson, Autism Spectrum News, December 30, 2024
In the autistic community, we often hear the phrase “Nothing about us without us.”
| |
|
|
On its surface, that seems like the ethical standard that those of us who are not autistic should commit to. It feels respectful for non-autistic clinicians, educators, and researchers like me to take our lead from autistic people. And bringing autistic advocates to the table is doable, as there are plenty who have the willingness and ability to lead. In fact, not doing so seems ableist.
That said, if we look beneath it all, strictly adhering to “nothing about us without us” may not be in the best interest of all those on the wide-ranging autism spectrum and those who care for them. In fact, if we’re talking about empowering the voices of the entirety of the community, outside advocacy is necessary for those who require round-the-clock support and significant care. If we paint everyone within this heterogeneous population with a broad brush, we’re leaving those with the most needs behind.
I am a physically disabled person and a wheelchair user. I identify as disabled and usually use identity first language. I travel and speak at conferences and have had the opportunity to advocate for many issues related to wheelchair users like me. So, what does this phrase, “nothing about us without us,” mean for me and the physically disabled community?
Before I can answer that question, there are some other important questions I need to ask: Do I really represent the broad, varied experiences and needs of the diverse population of physically disabled people? Do I represent quadriplegics? Should I place myself in a position to speak for someone who needs 24-hour assistance to do physical activities like eating, dressing, or toileting when I can manage these personal tasks on my own? Can I speak for someone with a fast progressive disease like amyotrophic lateral sclerosis (ALS) when my own condition is very slowly progressive?
I follow a number of people on social media with ALS who refer to themselves as “ALS Warriors.” While I rarely think about a cure for myself, many ALS Warriors think about a cure every day. The truth is my disabled experience is as different from someone with ALS as the experience of an autistic person with a PhD is to someone with autism and severe/profound intellectual disability.
For me, “nothing about us without us” is specific to people whose disability experience is close to mine.
I rarely hear this perspective from autistic advocates either at the conferences I go to or in the articles I read. What I hear is articulate, educated autistic advocates like the medical student I listened to at a conference last year suggest that they speak for the autistic population. Some even going so far as to say parents of autistic children “can’t speak” for their autistic children because they themselves aren’t autistic.
This begs the question for autism researchers and clinicians like me, ‘Who does the phrase “nothing about us without us” refer to when considering the needs of significantly disabled autistic people?’ If the data about severe autism is correct, almost one-third of the autistic population falls into the category of profound autism. It is beyond the cognitive abilities of individuals in this group, whose severe disability includes minimal language, to understand the phrase “nothing about us without us.”
As a disabled person and advocate, I think I must ensure that I am not speaking for people whose disability experience is very different from mine. Similarly, autistic people who are able to communicate and understand the phrase “nothing about us without us” shouldn’t speak for autistic people for whom this phrase is meaningless. Instead, I propose that for severely disabled autistic people, we broaden the phrase “nothing about us without us” to include parents. This will not happen unless autistic advocates recognize that they cannot speak for the entire autistic population and acknowledge that parents should be included in “nothing about us without us.”
Parents and caregivers are the people who are there at 3 a.m. when a profoundly disabled, non-verbal autistic person is having a very bad night, is not sleeping, and has become aggressive. Unfortunately, in the push by some autistic advocates to speak for the entire autistic population, caregivers are being left out of “nothing about us without us.”
My message is this: as disabled people, we should be careful about who we represent. In extremely heterogeneous populations like the autism community, we need to ask what “nothing about us without us” really means.
Link to the article here
| |
RFK, Jr. to head HHS & MAHA: | |
RFK Jr. sworn in as head of HHS following 52-48 Senate vote
By Emma Beavins and Dave Muoio, Fierce Healthcare, February 13, 2025
Robert F. Kennedy Jr. is now Health Secretary of the United States.
The Senate voted to confirm Kennedy 52-48 to lead the Department of Health and Human Services (HHS) on Thursday morning. Most Republicans voted in favor of Kennedy except for Kentucky Republican Mitch McConnell, who sided with Democrats in the vote.
Kennedy was sworn in on Thursday afternoon as the 26th Secretary of the U.S. Department of Health and Human Services (HHS) in the Oval Office by Associate Justice of the Supreme Court Neil Gorsuch.
Alongside the swearing in ceremony, President Donald Trump announced an executive order that establishes a Make America Healthy Again commission, which seeks to identify the remaining questions about childhood chronic disease, in its first 100 days.
"Thank you, President Trump, for your leadership, your confidence in me, and your deep concern for the health of the American people,” Secretary Kennedy said in a statement. “You have truly heard the calls of the millions of mothers who simply want the tools – and the truth – so they can make informed decisions for their children.”
“I have prayed each morning for the past two decades for God to put me in a position to solve the childhood chronic disease epidemic,” Kennedy continued, “and now, thanks to you Mr. President, we will make this promise a reality.”
Continued
| |
Trump's 'Make America Healthy Again' commission to target autism, chronic diseases
By Emma Colton, Fox News, February 13, 2025
President Donald Trump will sign an executive order on Thursday establishing the Make America Healthy Again Commission, which will be led by newly confirmed Health and Human Services Secretary Robert F. Kennedy Jr., Fox News Digital exclusively learned.
The commission will be chaired by Kennedy and will be "tasked with investigating and addressing the root causes of America’s escalating health crisis, with an initial focus on childhood chronic diseases," the White House explained to Fox News Digital.
Kennedy was confirmed as the nation's leader of the U.S. Health and Human Services on Thursday and was expected to be sworn in later in the afternoon. His commission will work to "restore trust in medical and scientific institutions and hold public hearings, meetings, roundtables" to receive input from health leaders.
The commission, Fox Digital learned, will focus on four policy directives to reverse chronic disease, including providing Americans transparency on health data to "avoid conflicts of interest in all federally funded health research;" prioritizing "gold-standard research on why Americans are getting sick" in all federally-funded health research; working with farmers to ensure food is healthy, as well as affordable; and expanding health coverage and treatment options "for beneficial lifestyle changes and disease prevention."
The commission initially will focus on childhood chronic diseases, such as autism and fatty liver disease, and also investigate adult chronic diseases, such as asthma and the U.S. average life expectancy compared to other nations.
RFK JR. VOWS HE WON'T TAKE CHEESEBURGERS AWAY, 'MY BOSS LOVES' THEM
Within 100 days of the commission's founding, it is expected to publish "an assessment that summarizes what is known and what questions remain regarding the childhood chronic disease crisis, and include international comparisons." Within 180 days, it is expected to "produce a strategy, based on the findings of the assessment, to improve the health of America’s children," Fox Digital learned.
Kennedy and Trump vowed on the campaign trail to "Make America Healthy Again," including directing their focus on autism among youths in recent years. The commission will investigate chronic conditions for both adults and children, including those related to autism, which the White House said affects one in 36 children.
Trump, in recent months, has cited autism stats while previewing his second administration, balking at the number of children currently diagnosed compared to just 25 years ago.
"When you look at, like, autism from 25 years ago, and you look at it now, something's going on," Trump said in December ahead of his inauguration. "Think of this: 25 years ago, autism, 1 in 10,000 children. Today it's 1 in 36 children. Is something wrong? I think so, and Robert and I, we're going to figure it out."
Trump also vowed while on the campaign trail in June that he would "establish a special Presidential Commission of independent minds who are not bought and paid for by Big Pharma, and I will charge them with investigating what is causing the decades-long increase in chronic illnesses."
TRUMP INNER CIRCLE SHARES MCDONALD’S MEAL AS DONALD JR. JOKES 'MAKE AMERICA HEALTHY AGAIN STARTS TOMORROW’
Read the full piece here
| |
What does HHS do? What to know as RFK confirmed as Trump's health secretary
As secretary, Kennedy will be responsible for food and hospital inspections, providing health insurance for millions of Americans and researching deadly diseases
By NBC Chicago Staff and Associated Press, February 13, 2025
Robert F. Kennedy Jr. was confirmed as President Donald Trump’s health secretary Thursday, but what exactly does the Health and Human Services Department do and what is his role?
As secretary, Kennedy will be responsible for food and hospital inspections, providing health insurance for millions of Americans and researching deadly diseases.
Among the agencies under the Health and Human Services Department are the Food and Drug Administration, the Centers for Disease Control and Prevention, and the National Institutes for Health.
Here's what to know:
What does the HHS Department do?
HHS is a massive Cabinet agency that oversees everything from drug, vaccine and food safety to medical research and the social safety net programs Medicare and Medicaid.
"The mission of the U.S. Department of Health and Human Services (HHS) is to enhance the health and well-being of all Americans, by providing for effective health and human services and by fostering sound, sustained advances in the sciences underlying medicine, public health, and social services," the department's website reads.
Which agencies are under HHS?
- Administration for Children and Families (ACF)
- Administration for Community Living (ACL)
- Advanced Research Projects Agency for Health (ARPA-H)
- Administration for Strategic Preparedness and Response (ASPR)
- Agency for Healthcare Research and Quality (AHRQ)
- Assistant Secretary for Technology Policy/Office of the National Coordinator for Health Information Technology (ASTP/ONC)
- Agency for Toxic Substances and Disease Registry (ATSDR)
- Assistant Secretary for Administration (ASA)
- Assistant Secretary for Financial Resources (ASFR)
- Assistant Secretary for Health (ASH)
- Assistant Secretary for Legislation (ASL)
- Assistant Secretary for Planning and Evaluation (ASPE)
- Assistant Secretary for Public Affairs (ASPA)
- Center for Faith-Based and Neighborhood Partnerships (CFBNP)
- Centers for Disease Control and Prevention (CDC)
- Centers for Medicare & Medicaid Services (CMS)
- Departmental Appeals Board (DAB)
- Food and Drug Administration (FDA)
- Health Resources and Services Administration (HRSA)
- Immediate Office of the Secretary (IOS)
- Indian Health Service (IHS)
- National Institutes of Health (NIH)
- Office for Civil Rights (OCR)
- Office of Global Affairs (OGA)
- Office of Inspector General (OIG)
- Office of Intergovernmental and External Affairs (IEA)
- Office of Medicare Hearings and Appeals (OMHA)
- Office of the General Counsel (OGC)
- Substance Abuse and Mental Health Services Administration (SAMHSA)
Continued
| |
‘Terrifying’: Public Health Experts React to Senate’s Confirmation of RFK Jr. to Lead HHS
By Chantelle Lee, TIME Magazine, February 13, 2025
The Senate confirmed Robert F. Kennedy Jr., one of America’s most notorious vaccine skeptics, to run the country’s leading health agency, the U.S. Department of Health and Human Services (HHS), on Thursday, sparking outrage among public health experts who worry that Kennedy will harm public health and further erode trust in science and medicine.
“I think it’s a sad day for America’s children. I think it’s a sad day for public health when someone who is a science denialist, conspiracy theorist, and virulent anti-vaccine activist is [leading] the biggest public health agency in the United States,” says Dr. Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, who has served on vaccine advisory committees for the U.S. Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration (FDA). “I think every Senator who voted for his confirmation should be ashamed of themselves for their unwillingness to stand up for the health of the American public.”
Kennedy, 71, was one of President Donald Trump’s most controversial Cabinet nominees. For years, Kennedy has spread medical disinformation, enraging experts in the field. He’s repeated the debunked claim that vaccines cause autism—even though research overwhelmingly proves that vaccines are both safe and effective—and has made controversial statements about raw milk and fluoride in water. During his confirmation hearings, he faced heated questioning by Senators over his anti-vaccine views, flip-flopping stance on abortion, and previous support for some conspiracy theories, such as his assertions that Lyme Disease and COVID-19 were engineered bioweapons. He appeared unfamiliar with certain issues he would oversee as the head of HHS, at times seemingly confusing Medicaid and Medicare. All the same, Kennedy was confirmed by a vote of 52 to 48, with Sen. Mitch McConnell of Kentucky—a polio survivor—the only Republican who voted against his confirmation.
Public health experts first sounded the alarm when Trump announced Kennedy as his nominee to lead HHS back in November. As head of HHS, Kennedy will oversee health agencies like the CDC and the FDA.
At the forefront of experts’ concern is the influence Kennedy would have over vaccines. Kennedy tried to distance himself from his previous anti-vaccine statements during his confirmation hearings, saying that he’s not “anti-vaccine” but “pro-safety,” and he has said that he and the Trump Administration wouldn’t take vaccines off the market. But experts cast doubt on whether the Administration would hold true to that statement, and many worry that Kennedy could appoint people to agencies like the FDA and CDC who could impede or revoke vaccine approvals, not only limiting access to but also sowing distrust in a powerful public health tool.
Dr. Rob Davidson is an emergency physician in Michigan and executive director of the Committee to Protect Health Care, which had circulated a petition garnering more than 22,000 signatures from physicians calling on the Senate to reject Kennedy. Davidson says he worries about how Kennedy will respond to emerging diseases, such as H5N1, more commonly known as bird flu. In addition to his anti-vaccine rhetoric, Kennedy has previously suggested putting a pause on infectious disease research, sparking backlash from many public health experts.
“He’s just a dangerous individual when it comes to public health,” Davidson says. “It’s dangerous to have a guy who’s led [the vaccine skepticism] movement being the head of this agency, the mouthpiece of the U.S. government when it comes to public health. So that is truly terrifying.”
“I think a lot of lives are at risk potentially because of this person running this agency,” Davidson continues.
Read the full article here
| |
Reminder: Monday is Presidents' Day | |
VOR will be closed in remembrance of our great American presidents. | |
|
Action Alert:
Section 504 Protections in the Crosshairs:
| |
Texas v. Becerra: What it is and How You Can Help Stop the Attack on Section 504
From DREDF. org, February 13, 2025
What is Texas v. Becerra?
Texas v. Becerra is a court case in Texas. A group of 17 states have sued the United States government. The states are asking the court to get rid of Section 504 and its new rules that protect people with disabilities from discrimination in health care and human services.
What is Section 504?
Section 504 is an important law that protects people with disabilities. Section 504 says you can’t discriminate against disabled people if you get money from the United States government. To discriminate means to treat people badly because of who they are. Section 504 says you cannot treat people badly because of their disabilities.
Section 504 has rules that explain what disability discrimination is. The rules say that places like schools, hospitals, and doctors’ offices have to include people with disabilities. The rules say what these places have to do to include people with disabilities. Anyone who gets money from the United States government to serve the public or do business has to follow the rules.
The United States government finished the first Section 504 rules in 1977. Many disabled people protested so that the government would make the rules strong.
The United States government updates the Section 504 rules over time. The government just finished updating the rules in 2024. Many disability advocates wrote to the government about what to put in the rules. The updated rules are stronger and have more examples about what disability discrimination is.
Why is Section 504 important?
Section 504 covers all parts of society that get money from the United States government. Section 504 and its rules are very important, especially in education and healthcare. Here are some ways that Section 504 and its rules help us. The rules in Section 504 say that:
- Schools must include students with disabilities and help them learn.
- Doctors and schools must have sign language interpreters for people who are Deaf and Hard of Hearing who sign. Videos must have captions.
- Doctors must give clear information to disabled people. This includes people with intellectual and developmental disabilities.
- Websites for schools and hospitals must work for people who are blind and low vision.
- Doctors and hospitals cannot stop helping someone because they have a disability.
- Doctors and hospitals must have tools and machines that work for wheelchair users. This includes machines that check for cancer.
What Do the 17 States Want?
17 states sued the United States government. They asked the court to get rid of Section 504. The states disagree with a few things in the updated Section 504 rules. But the lawsuit asks the court to get rid of all the updated rules – and to get rid of Section 504 itself, not just the rules they disagree with. The lawsuit says that Section 504 goes against the United States Constitution. The lawsuit says that no one should have to follow any part of Section 504. If the 17 states win, this would be a disaster for people with disabilities.
| |
|
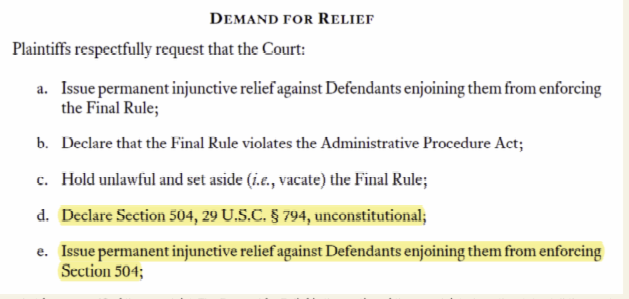
The above image is a screenshot from page 43 of the complaint. The Demand for Relief is the section of the complaint where the states tell the court what they want the court to do. Text reads: Demand for Relief. Plaintiffs respectfully request that the Court: a. Issue permanent injunctive relief against Defendants enjoining them from enforcing the Final Rule; b. Declare that the Final Rule violates the Administrative Procedure Act; c. Hold unlawful and set aside (i.e., vacate) the Final Rule; d. Declare Section 504, 29 U.S.C. § 794, unconstitutional; e. Issue permanent injunctive relief against Defendants enjoining them from enforcing Section 504;”
What Will Happen Next?
The judge set a schedule for the case. The 17 states and the United States government will give the court papers on February 25, 2025, about what should happen with the case. Other states that support Section 504 may want to file their own papers with the court.
Disability groups may want to file amicus briefs. Amicus briefs are papers that people or groups can send to a court during a court case. The people or groups who send amicus briefs are not part of the court case. They are not the people suing or being sued. People and groups use amicus briefs to explain what decision they want the court to make, and why.
After the court has all the papers, it will make a decision about the case.
What Can I Do to Help?
Tell Your State Attorney General to Stop Attacking Section 504
You can do more if you live in one of the states that is bringing the case. You can ask your state Attorney General to drop out of the case. You can ask them to drop out of the case in a meeting, in writing, or on the phone. You can ask by yourself or in a group. A group of people can be powerful. You may find a group in your community. You can ask disability groups like your local Center for Independent Living or a chapter of the Arc.
Continue here for more information about how you can help
| |
In a new lawsuit, 17 states sue to do away with 504 protections
By Staff. The Education Room, February 11, 2025
A high-stakes lawsuit, Texas v. Becerra, is currently making its way through the courts, threatening crucial protections for people with disabilities under Section 504 of the Rehabilitation Act. Seventeen states have challenged the federal government’s updated rules, putting at risk decades of legal safeguards that ensure accessibility in education, healthcare, and other public services.
In this case, a coalition of 17 states ( Alaska, Alabama, Arkansas, Flordia, Georgia, Indiana, Iowa, Kansas, Louisiana, Missouri, Montana, Nebraska, South Carolina, South Dakota, Texas, Utah, and West Virginia) has sued the U.S. government, arguing that Section 504 is unconstitutional and should be eliminated. If successful, the lawsuit could dismantle essential protections that prevent discrimination against people with disabilities.
What is Section 504?
Section 504 of the Rehabilitation Act, first implemented in 1977, prohibits discrimination against individuals with disabilities by entities that receive federal funding. The law mandates that schools, hospitals, and other federally funded institutions provide equal access and accommodations to disabled individuals. The U.S. Department of Health and Human Services (HHS) recently updated the rules under Section 504 in 2024, incorporating stronger protections based on extensive input from disability advocates.
These regulations require schools to provide appropriate support for students with disabilities, ensure that hospitals have sign language interpreters, mandate captioning for videos, and require accessible medical equipment for wheelchair users.
Why the Lawsuit Matters
The states behind Texas v. Becerra argue that the federal government overstepped its authority in implementing the updated Section 504 rules. However, rather than targeting specific provisions, the lawsuit seeks to dismantle Section 504 in its entirety. If successful, this case could strip away fundamental protections, making it easier for discrimination against disabled individuals to go unchallenged.
What Comes Next?
The legal process is already underway. By February 25, 2025, both the 17 states and the federal government will submit legal briefs outlining their positions. Other states that support Section 504 may also file documents in its defense. Disability advocacy organizations are expected to submit amicus briefs—legal arguments from non-parties explaining the broader implications of the case.
Once the court reviews all submitted documents, a ruling will be issued. The outcome will shape the future of disability rights and accessibility laws in the United States.
Link to the article here
Download the complaint here
Note: While this case may have originated as a lawsuit to deny the rights of transgender individuals, it has the scope to eliminate Section 504 protections for people with I/DD and autism.
| |
Education in the Crosshairs: | |
Push To Dismantle Ed Department Fuels Worries About Special Education
By Michelle Diament, Disability Scoop, February 11, 2025
As President Donald Trump doubles down on his pledge to shutter the U.S. Department of Education, the ramifications for students with disabilities could be severe, advocates say.
Trump says that the Education Department is the next target in his administration’s efforts to weed out wasteful spending. Recent reports indicate that the White House is considering an executive order designed to dismantle the department and the president, who has said he wants to close the agency, told reporters that he’s directed Linda McMahon, his nominee for education secretary, to “put herself out of a job.”
While experts say that closing the agency would require an act of Congress, advocates are warning that any efforts to weaken the Education Department could have an outsized impact on the nation’s 7.5 million special education students.
“We have deep concern as we see or hear nothing that assures us the administration understands and intends to carry out its obligation to protect our kids or understands that (the Education Department) has an obligation to assure our kids get the services and supports they are entitled to under the law,” said Denise S. Marshall, CEO of the Council of Parent Attorneys and Advocates, or COPAA, a nonprofit that advocates for the rights of students with disabilities and their families.
While federal laws including the Individuals with Disabilities Education Act and Section 504 of the Rehabilitation Act guarantee students with disabilities certain rights in schools, the Education Department plays a major role in ensuring that these laws are implemented.
“The interplay of the federal laws that serve and protect our children is complex, there must be expert personnel who work to carry out the statute’s requirements,” Marshall said. “IDEA delegates distinct duties to the secretary of education and the law obligates the department to provide oversight, technical assistance and more so that states can fulfill their obligation to provide a free, appropriate public education to every student with a disability.”
“We must recognize that students with disabilities, such as autism, deserve the same opportunities to succeed as their peers, and that specialized educational support is not a luxury, but a right,” said Christopher Banks, president and CEO of the Autism Society of America. “Removing federal oversight could undermine accessibility, equity and inclusion, leaving students vulnerable to disparities in quality education and long-term opportunities.”
Read the full article here
| |
How students with special needs could be impacted if Trump dismantles Dept. of Education
By Amanda Chin, Fox News 17 Nashville, February 7, 2025
President Donald Trump says he plans to dismantle The U.S. Department of Education.
Some question how this would affect special needs students, most of whom rely on federal funding.
The former Assistant Commissioner of Special Populations for the Tennessee Department of Education says while the rights and protections of students with disabilities are protected by federal law, it's a matter of what authority the federal government would continue to have along with local authority.
Eleese Meschery has three boys. One of her sons is autistic and dyslexic, and he relies on federal funding through the Individuals with Disabilities Education Act (IDEA) to help him get the support and services he needs at school.
“If this is taken away and it’s left up to the states how are you gonna support my kids? Where is the accountability going to be?” asks Meschery.
So, what will happen to this IDEA funding?
According to a Special Education Support Organization, Tennessee STEP, around 130,000 Tennessee families rely on special education services.
“What we’re not sure of is without the enforcement, without the guidance from the U.S. Department of Ed, what do states need to be doing? What do they need to be looking at?” asks Theresa Nicholls, the former Assistant Commissioner for Special Population for the Tennessee Department of Education.
Nicholls says there are still questions about how IDEA would be implemented and how it’s going to be enforced.
“What we’re not sure right now is if the US Department of Ed is not the agency that’s sending those funds, who’s going to do that?” says Nicholls.
Continued
| |
Trump's plan to dismantle education department sparks fears for special needs kids
By Karina Hollingsworth, Fox News San Antonio, February 8, 2025
President Donald Trump is putting action behind his words and making good on a promise he made in 2023 pledging to dismantle the U.S. Department of Education. The pledge has sparked concern in some, while others are supporting the President.
Ovidia Molina, the president of the Texas State Teachers Association says dismantling the department puts all students at risk, especially the most vulnerable.
“We have special education programs that our children with disabilities who need more assistance, we would get funding for that to be able to give resources to our students,” Molina said.
Meagan Kirk, a mother of eight, is scared to lose those resources because three of her children have disabilities.
“If the funding is going to be cut special ed training is going to be cut,” Kirk said. “Special ed training is important.”
Kirk says her 8-year-old son Jett’s education is already suffering because he was recently diagnosed with a brain tumor.
“He is homebound,” Kirk said. “I can see that program being cut immediately. Oh, the kid’s too sick to come to school so he’s probably too sick to learn. We’re not going to pay a teacher to go to the house.”
The mother of 8 is also concerned about cuts to technology grants that helped provide her non-verbal daughter Maddie-Joe a communication device.
“That is her way of communication,” Kirk said. ‘If schools lose those grants, and that funding, that’s literally taking her voice away.”
Continued
| |
What Happens to Students With Disabilities if the Department of Education Were Dismantled?
By Heather Eckner, The Tennessee Tribune, February 11, 2025
The U.S. Department of Education plays a crucial role in ensuring that all students, regardless of background or ability, have access to a quality education. For students with disabilities, the Department has been instrumental in creating programs, policies, and frameworks that ensure equitable educational opportunities.
For students with disabilities, the consequences could be significant and detrimental to their ability to succeed in school and beyond. Here’s what’s at stake.
(1) Loss of Specialized Support and Services
One of the most important functions of the Department of Education is to oversee and enforce laws like the Individuals with Disabilities Education Act (IDEA), which mandates that students with disabilities receive free appropriate public education (FAPE). If the Department were to be dismantled, enforcement of IDEA and other related laws could become fragmented or inconsistent.
States are already tasked with a significant portion of the administration of special education to eligible students with disabilities, meaning, there is already a great deal of “local control” afforded in a system structure that includes a federal department. The loss of a central federal department focused on education would likely cause a significant cycle of confusion and chaos.
(2) Increased Risk of Inequity Across States
Currently, the U.S. Department of Education distributes funding to states across a number of programs, including Title I and the IDEA, which support at-risk students and students with disabilities. The Department also provides guidelines and ensures that schools across the country adhere to federal laws regarding accessibility and inclusion. In the absence of a national oversight body, the quality of services for students with disabilities could vary dramatically from state to state. Some states may have strong systems and programs for special education, while others may lack the infrastructure, funding, or training necessary to adequately support students with disabilities.
This could create an exacerbated patchwork system where students with disabilities in certain regions are left behind, while others have access to cutting-edge resources and opportunities. The inequality that would result could leave many students vulnerable, further exacerbating the disparities in educational outcomes for this population.
(3) Weakened Advocacy and Representation
The U.S. Department of Education is not just a regulatory body; it also plays a vital role in advocacy for marginalized groups, including students with disabilities. Without this national platform, students and families would likely struggle to have their voices heard in policy discussions at the federal level. Moreover, advocacy groups that work to advance the rights of students with disabilities might face more difficulty engaging with policymakers and securing necessary changes.
Dismantling the Department could also result in a decrease in funding for special education programs. Without a strong federal presence, local education agencies may struggle to meet the needs of students, particularly those with the most complex disabilities. Federal grants that support adaptive technologies, training for special education teachers, and other specialized resources might be eliminated, leaving school districts to pick up the slack—often without the means to do so.
(4) Potential Erosion of Civil Rights Protections
The Department of Education also plays a role in upholding the civil rights of students with disabilities. It ensures that students are not discriminated against based on their disability and that they have access to the same educational opportunities as their peers. If the Department were dismantled, oversight of these protections could weaken, allowing discrimination or exclusion to go unchecked. Students with disabilities could face increased challenges in securing the accommodations they need to participate in school activities, leading to further isolation and disadvantage.
Continued
| |
Minnesota - Disability advocates express concern over proposed Walz budget cuts
By Megan Zemple, KTTC Mews, February 6, 2025
Some Minnesota disability advocates are expressing concerns about Governor Tim Walz’s budget proposal.
On January 16, Walz rolled out the budget which included cutting the statewide sales tax by .075%. The plan would also close certain “tax loopholes,” increase fraud oversight, and curb “unsustainable growth in spending in the programs that drive the structural deficit.”
He said if the budget proposal is passed, it would leave $2.1 billion in 2026-27 and $355 million in 2028-29.
It also included reducing state Medicaid waivers which is money that helps people with disabilities pay for services like home care. The waivers are funded through state and federal funds.
“The budget slows growth of disability waivers, and Health and Human Services spending more broadly while maintaining Minnesotans access to services, reductions to waivers total $1.3 billion over the next four years, capping automatic inflation adjustments at 2% per year which will save the state more than $600 million over the next four years,” Minnesota Budget and Management Commissioner Erin Campbell said.
PossAbilities is a nonprofit organization in Rochester that serves individuals with disabilities. It helps them things like with home care, employment and life enrichment. It currently has 300 people that receive waivers, and they are the main source of funding.
PossAbilities Executive Director Susan Mackert said she is concerned about the possible cuts to the waivers.
“Waivers are the lifeblood for people with disabilities and their families,” Mackert said. “It was disappointing to see that in his budget that he’s calling for not just financial cuts but policy cuts that contribute to financial cuts, but I can only imagine he’s preparing for potential federal cuts.”
Mackert said the waivers also impact how much they pay employees.
“At PossAbilities, we work really hard to improve and we have improved wages, and the environment but also to keep things like administration low so the money that comes in from waivers goes to where it should and that’s to our direct support professionals,” she said.
Mackert said she hopes Walz and legislators can find a better solution.
Continued
| |
Minnesotans with disabilities say proposed budget cuts would ‘bring us backward’
By Jessie Van Berkel and James Walsh, The Minnesota Star Tribune, February 5, 2025
| |
Sumukha Terakanambi’s disability services waiver paid for the lift the Lakeville resident uses to get out of bed and the care that allows him to live in his family’s home.
For Steve Reinardy, whose eye disorder keeps him from driving, his waiver covers the transportation he needs to get to his job and doctor’s appointments.
Tim Gross has seen his son Ben, who has Down syndrome, develop life skills using waiver-funded training that allows him to remain in his own Duluth apartment.
They are among the Minnesotans pushing back against Gov. Tim Walz’s proposed measures to reduce planned increases in state spending on the Medicaid waivers that support tens of thousands of people with disabilities. The governor’s recent proposal, paired with fears over the Trump administration’s next steps on Medicaid, has many of the state’s most vulnerable residents and the people who care for them on edge.
“The uncertainty is incredible,” Gross said, who fears what the future holds for his son if government officials scale back services and he’s no longer around to help. “We have to count on decisions made in St. Paul and in D.C. that truly affect us immediately.”
Threats to Medicaid services have prompted a flurry of local and national action. Disability advocates are meeting to discuss the governor’s proposal and developing plans to push back, and service providers are sending messages urging lawmakers to oppose waiver spending cuts. Meanwhile, national advocacy groups are warily awaiting President Donald Trump’s next moves as U.S. House Republicans eye Medicaid cuts.
Whether Minnesota lawmakers will support the DFL governor’s proposed changes remains unclear. Senate Human Services Chair John Hoffman, DFL-Champlin, quickly decried Walz’s plan, saying it threatens to undermine the state’s progress in serving people with disabilities and aging residents.
“These measures do not align with the Minnesota way — a way that prioritizes compassion, equity, and support for those who need it most,“ Hoffman said in a statement. ”Balancing the state budget is a necessary responsibility, but it cannot be done at the expense of those who have no other safety net.”
Underlying Walz’s proposals are a looming budget deficit in 2028 and Medicaid spending on disability services that is far higher than other states' and growing faster than anticipated.
“We are not changing that Minnesota is a generous state,” Walz said when he unveiled his budget, but warned that spending on those services would balloon to one-eighth of Minnesota’s budget in 2029, and half of the budget by 2035. “This one has to be addressed and this budget does that. It does it responsibly, it does it morally, it does it ethically.”
But several people who run disability service programs have a very different description of Walz’s plan: They said he is balancing the budget “on the backs of people with disabilities.”
Continued
| |
Arizona - Disability advocates call on legislature to close $122M funding gap at Division of Developmental Disabilities
By Colleen Sikora, NBC 12 News, February 12, 2025
The Developmental Disability community in Arizona is calling for the legislature to take action as the state division that serves some 60,000 people is running out on Monday.
The Division of Developmental Disabilities is facing a $122 million shortfall in the coming months.
"Those services include things like day programs in-home services, nursing care, therapies, and it ranges from for members ranging from zero to 100 so it affects the entire disability community in Arizona," Brandi Coon said.
Coon, who's a disability advocate and a mother caregiver herself, calls the funding critical.
"We need to have a gap funding option in order for services to the DDD population to not run out in spring of this year," Coon said.
Governor Katie Hobbs asked the legislature for additional money as a stopgap because of what she says is caseload growth.
"We need to keep these services in place for these families who need them," Hobbs said.
A bill introduced earlier this week by Democrat Representative Nancy Gutierrez would cover the $122 million shortfall, but that bill has not been heard in committee.
Wednesday afternoon, House Appropriations Committee Chair David Livingston offered some hope: A budget for next year could be done before funding runs out in a few months.
"It's something that will have to be fixed when we do a budget, and hopefully we'll be able to do that budget and sine die in April and not affect the DD community in their payments starting May 1," Livingston, a Republican, said. "That is the goal of this chairman. That is the goal of I think I remember this body, and if it's not, it should be."
However, Coon wants to see the bill Gutierrez introduced be heard in the committee when it meets again next week.
Continued
| |
Kentucky - Fighting for Frankie: A Louisville family's 700-mile journey for son with severe autism
A Louisville family's sharing their heartbreaking journey in their fight to keep their 15-year-old son with severe autism close to home.
Frankie Moldoveanu has profound, level 3, autism, and is also nonverbal. In recent years, he's become more aggressive and unpredictable, causing harm to his family, and with two young sisters at home, his parents were left with no choice but to find a place that could take care of Frankie full-time.
They quickly discovered there was no such place in Kentucky.
Their best option was hundreds of miles away.
On Jan. 28, more than a dozen of Frankie's friends and family gathered at UofL Health's Peace Hospital to send him off on his next journey.
"You ready to go?" his mom asked, as he walked down the hospital stairs to a crowded lobby.
His months-long stay at Peace had come to an end. It was a familiar place for Frankie. He'd been there before. But this time, he wasn't going home. At least, not to the one he knows.
They'd packed their SUV for the 11-hour journey to Wichita, Kansas; one they'd looked forward to and dreaded all at the same time.
The next morning, they rolled up to the entrance of Heartspring, a place where children with severe neurodevelopmental disorders can receive the care they need to become more independent. More than 500 kids living with autism, ADHD or other learning disabilities receive therapeutic care here every year. Kids from California, Kentucky, Montana and Texas.
In all, children from 17 states.
Some use the outpatient services like speech therapy, and occupational and behavioral care. Other kids need that care around the clock.
"Every single day we get phone calls from families desperate for services," Cara Rapp, the admissions director at Heartspring said.
Rachel Moldoveanu and her husband, Bob, made that call back in the summer, in search of a place Frankie could call home, when theirs was no longer a safe place. He's grown too big and too strong to control. And there are just a handful of facilities across the country that can provide this type of specialized care, for Frankie and kids like him.
Currently, Heartspring is home to about 80 kids, who live and go to school on campus.
"I am very thankful for Heartspring and Kansas, but I am very sad that I have to leave my child 700 miles away and that's not an easy thing to do as a mom," Rachel said.
Read the full article here
| |
Kansas committee proposes doubling down to fix notoriously long I/DD waitlist
By Jack Harvel, The Topeka Capital-Journal, February 10, 2025
Kansas's Committee on the Social Services Budget recommended further reducing the state's waitlist for Intellectual/Developmental Disabilities waiver after a big investment in the program last year.
Applicants can be on a waitlist for up to a decade before they're finally able to access Medicaid-funded services. The waiver can pay for things like adult daycare, overnight care, specialized medical care and specialized employment.
Last year Kansas added 500 additional slots to the number of people who can receive services through the waiver and capped the number of people that can be on the waitlist at 4,800. It similarly added slots to the Physical Disability Waiver program, which suffered similar but less acute problems with its waitlist, and it has functionally solved its issues.
"The good news is that KDADs is saying that they're going to clear the entire waiting list," said Rocky Nichols, executive director of the Disability Rights Center of Kansas. "But the bad news with that is the reason why they can clear the entire PD waiting list is because they've lost so many people."
Continued
| |
|
Kansans with intellectual and developmental disabilities have a new chance for help
By Whit Downing, The Kansas City Star, February 10, 2025
I spent eight years on the Kansas Intellectual/Developmental Disability waiver waitlist.
In my years on the list, I experienced more psychiatric hospital stays than I can count or even remember. I survived a suicide attempt. I wore my family out emotionally and physically as they tried to help me navigate a world that often felt unaccommodating and overwhelming. There were times when my meltdowns led to the police being called — and then I ended up in the back of a police car, even though I did nothing illegal or because I was a danger to anyone. I just lacked the proper supports that could have de-escalated the situation. I’ve spent countless hours sitting in emergency rooms, waiting for help that often felt out of reach.
The truth is, so much of that pain, chaos and trauma could have been avoided if I’d had the right support at the right time I needed it. Proper funding for mental health waiver services doesn’t just improve lives — it saves them. It gives people with intellectual and developmental disabilities and their families the chance to thrive rather than just survive.
There are more than 4,300 Kansans who are on the I/DD waiver waitlist. That’s 4,300 names, 4,300 stories, 4,300 lives placed on hold. These are not just numbers on a Kansas Department for Aging and Disability Services spreadsheet. They are real people with dreams, struggles and potential. I know because I was one of them.
For those on the waitlist, each day that passes is another day stolen from them — not by chance, but by a broken system that has the potential to be fixed.
This year, we have a chance to change that. Momentum is building at the Kansas State Capitol. Recently, the House Committee on Social Services Budget took a critical step toward ending the waitlist crisis by unanimously recommending funding to support the following plan, which I am in full agreement: funding for another 500 Kansans to receive I/DD waiver services, capping the waitlist so it can’t grow over 4,300, and making strides so we can start a new waiver in Kansas called the Community Supports Waiver, which is a small waiver that would allow people like me to receive minimal supports in our communities.
This is an amazing step forward, but we cannot stop here. We need every state lawmaker to support this request, vote for it and send it to Gov. Laura Kelly’s desk for her signature.
Continued
| |
'We are struggling': Medicaid home caregivers want Texas lawmakers to increase wages
By Madeline Figuelredo, The Austin American-Statesman, February 10, 2025
Thomas Greenwell wakes up each morning and gets ready twice — he goes through the motions of brushing teeth twice, doing hair twice and getting dressed twice — once for himself and once for his client, Edgar.
Greenwell is a community attendant in Pearland, south of Houston, who described his work as a full-time, hands-on effort. “Every single daily task someone would do for themselves, I do for myself and then I also do with Edgar,” Greenwell said.
But Greenwell doesn’t know how much longer he will be able to afford to take care of Edgar as a community-based care provider under Medicaid. He makes $10.60/hour, a wage set by the Legislature in 2023.
The attendant care wages are not sustainable at all,” the 19-year-old Greenwell said.
He lives with his family but said he has been hoping to move out for some time. “In Pearland, rent alone for a small apartment would take up both my monthly paychecks — forget taking into account gas, food or utilities,” he said.
The Legislature will revisit attendant wages in this spring’s legislative session as caregivers and advocacy groups push for more competitive and livable wages.
State Rep. Suleman Lalani, D-Sugar Land, who is also a physician, has introduced a bill that would set a minimum wage of $15 per hour for personal attendants under Medicaid and other Texas Health and Human Services programs.
“We owe care providers the opportunity to have a good quality of life that allows them to put food on the table,” Lalani said. “When you look at the numbers, people are making more money working at fast-food restaurants and grocery stores than the people who are breaking their backs taking care of fragile communities.”
Lalani said the low wages for attendant positions have fueled worker shortages and gaps in care that put preventive care on the back burner and lead to greater expenses down the line in hospitalizations and complications.
Continued
| |
|
Please share this offer with your loved one's
Direct Support Professionals!
VOR ❤️s OUR
DIRECT SUPPORT PROFESSIONALS!
Our loved ones' caregivers are essential to their health, safety, and happiness.
In appreciation of their good work and kind hearts, VOR offers free digital memberships to any DSP who would like to receive our newsletter.
We encourage our members to speak with their loved ones' caregivers to extend this offer of our gratitude.
If you are a Direct Support Professional interested in receiving our newsletter and e-content, please write us at
info@vor.net
with your name, email address, and the name of the facility at which you work. Please include the name of the VOR member who told you of this offer.
| |
|
What's Happening In Your Community?
Is there an issue in your loved one's home that you need help with?
Do you have information or a news story you would like to share?
Is there legislation in your state house that needs attention?
Contact us at info@vor.net
| |
|
So far this year, 2,243 bills have been introduced in the 119th Congress.
Only a very few of these bills have anything to do with people with I/DD or autism.
As yet, no text or summaries have yet appeared on the congressional website, so we cannot say if we support or oppose the bills.
Please stay tuned.
| |
836 South Arlington Heights Road #351
Elk Grove Village, IL 60007
Toll Free: 877-399-4867 Fax: 877-866-8377
| |
FACEBOOK: /VOR ----- TWITTER: @VOR_NET ----- YouTube
| | | | |