|
March is
Developmental
Disabilities
Awareness
Month
Are Your Members of Congress Aware of That?
| |
|
VOR's Weekly News Update
VOR is a national non-profit organization
run by families of people with I/DD and autism
for families of people with I/DD and autism.
| |
|
Contact Your Governor!
Last week, we sent out snail-mail letters to the Governors of all 50 states, asking to protect the people of their state by speaking with their Members of Congress and asking them to say
NO
to the proposed $880 Billion cuts to Medicaid
Please click here to download VOR's Letter
If these cuts are enacted, governors will be the ones to bear the initial burden. Their state budgets, already strapped for funds for Medicaid services, will be severely reduced. Hospitals will become overcrowded. Many will be forced to close through lack of funds.
And we all know what will happen to DD Services...
We need you to join us, by reaching out to your governor's office to tell your story, and to tell how cutting Medicaid would affect your family, and your loved ones and your state.
Your governor's contact can be found here
Once on their website, look for information on how to contact them. It may be a phone number, or an email address, but most likely there will be an online form to fill out. You may or may not be able to attache our VOR's letter, or you may paraphrase parts of it.
But please, reach out to your state office, and to the providers and administrators of the residential facilities that provide services for your loved ones, and ask them to speak to your governors, your members of the House of Representatives and Senate to demand that Congress
MAKE NO CUTS TO MEDICAID!
| |
|
Please join us on Capitol Hill
May 12-14, 2025
VOR's Annual Legislative Initiative
Washington, D.C.
| |
|
We will meet in D.C. on May 12th - 14th
for meetings with
Congressional Staff and Federal Agencies
to discuss issues of critical importance to
individuals with severe or profound I/DD and autism
and their families.
This year's topics are expected to include:
Preventing Cuts to Medicaid
and
Rebuilding and Supporting our DSP Workforce
This event is open to all members of VOR
Please register early, to reserve your spot
Registration is free until March 15, 2025
So please register now!
To register for the Legislative Initiative,
Please Click Here
| |
Unable to join us in D.C. this year?
You can still help by becoming a sponsor!
We are still far short of our goal for sponsors for this event!
This is a critical time for our families.
The actions taken by Congress and the Administration
in the next few months could impact the lives of
hundreds of thousands of people with I/DD and autism in the years to come.
Please help us help.
Diamond - $ 5,000
Platinum - $ 2,500
Gold - $1,000
Silver - $ 500
Bronze - $ 250
Advocacy Hero - $ 100
Friends & Families - (Other amounts)
| |
Any and all gifts are welcome | |
Protecting Medicaid from $880 Billion Cuts: | |
As G.O.P. Eyes Medicaid Cuts, States Could Be Left With Vast Shortfalls
By Noah Weiland and Sarah Kliff, The New York Times, February 25, 2025
House Republicans hunting for ways to pay for President Trump’s tax cuts have called for cutting the federal government’s share of Medicaid spending, including a proposal that would effectively gut the Affordable Care Act’s 2014 expansion of the program.
Cutting Medicaid spending, which is expected to be central to fulfilling the budget plan that House Republicans adopted Tuesday night, could result in millions of Americans across the country losing health coverage unless states decide to play a bigger role in its funding.
Federal and state governments share the costs of Medicaid, which is a public health insurance program largely for low-income people.
Republicans are considering lowering the 90 percent share that the federal government is required to pay to states that enroll participants in the expansion. The change could generate $560 billion in savings over a decade, money that Republicans want to use toward extending Mr. Trump’s 2017 tax cuts, which are set to expire at the end of 2025. Extending the tax cuts is expected to cost $4.5 trillion, meaning Republicans will have to find savings beyond Medicaid from a long menu of options.
A move to lower federal spending on the Medicaid expansion population could effectively gut the program. Around 10 states that have expanded their programs have so-called trigger laws that reverse the Medicaid expansion if the federal government decreases funding for the population.
Among those who qualified for Medicaid under the expansion was Jeannie Brown, a 60-year-old part-time bus driver for the public school system in Belgrade, Mont. Ms. Brown went more than five years without health insurance beginning in 2009, avoiding medical care as her health deteriorated and she cared for her disabled granddaughter.
Ms. Brown, who makes around $25,000 each year, had been trapped in the so-called coverage gap, with a salary too high for Medicaid, and too low for a heavily subsidized Obamacare plan.
After Montana lawmakers voted in 2015 to take up the Affordable Care Act’s option to expand Medicaid to cover more adults, Ms. Brown enrolled. She began to see a primary care doctor, and Medicaid paid for hand surgeries, knee replacements, a double mastectomy and her inhaler, she said.
“Being a caregiver is extremely exhausting, especially with someone who has a lot of health needs,” she said last week from a children’s hospital in Colorado, where her granddaughter had been flown for emergency care. “If I didn’t have the preventative care I needed, I’d be in a much worse place physically. I’d probably be disabled.”
The move to pare back the federal government’s financial commitments to Medicaid could profoundly reshape how it shares responsibility with states to offer health care to some of the poorest Americans, as well as the providers and nursing homes that care for them.
The change could leave the 40 states that participate in the Obamacare program with a difficult set of choices. They could shoulder the extra costs to preserve Medicaid coverage for millions, make cuts to coverage or look for cuts from other large government programs to offset the reduction in federal funds.
The change would amount to a “massive transfer of the financial responsibility from the federal government to states,” said Daniel Tsai, who oversaw Medicaid under former President Joseph R. Biden Jr.
“You’d have states having enormous budget holes making decisions between how to do the right thing to keep people covered” and how to preserve other programs, he said. “States are going to be cash strapped.”
Medicaid now funds almost half of all births in the United States, and represents more than half of spending on long-term care. More than 70 percent of Americans say they want Medicaid to stay as it is, according to a survey conducted last year by KFF, a nonprofit health policy research group.
Read the full article here
|
What Can House Republicans Cut Instead of Medicaid? Not Much.
The math of the G.O.P.’s goals makes the move almost unavoidable.
By Margot Sanger-Katz and Alicia Parlapiano, the New York Tmes, February 25, 2025
he House passed a budget resolution Tuesday night after Speaker Mike Johnson persuaded several Republican lawmakers, including those who have expressed reservations about possible Medicaid cuts, to support the bill.
In theory, the budget, which kicks off the process of passing an extension of tax cuts enacted in 2017 and up to $2 trillion in spending cuts meant to partly offset them, could become law without significant cuts to Medicaid. But it won’t be easy.
That process has a few more steps: For one, the Senate has to adopt this budget resolution. Then both houses of Congress will also need to write and pass legislation that follows its instructions.
The budget resolution itself is silent on whether Congress cuts Medicaid, which provides health coverage to 72 million poor and disabled Americans. But it instructs the House Energy and Commerce Committee, which has jurisdiction over the program, to cut spending by $880 billion over the next decade. If the committee can’t save at least that much, the entire effort could be imperiled because of the special process Congress is using to avoid a Senate filibuster. Ten other committees have their own instructions to follow, though none have been assigned with cutting nearly as much.
It’s not so simple as finding the cuts elsewhere. The special process, known as budget reconciliation, means Republicans will have to find all $880 billion from within the Energy and Commerce Committee’s jurisdiction. That leaves them with fewer options than one might think.
Continued
| |
71 percent of Trump voters oppose Medicaid cuts: Poll
By Jared Gans, The Hill, February 25, 2025
Most President Trump voters say they oppose any cuts to Medicaid as Republican lawmakers wrestle with how to reach up to $2 trillion in budget cuts through their reconciliation bill, a poll released Monday found.
The poll from Hart Research conducted for the nonprofit Families Over Billionaires, which advocates in opposition to tax cuts for the wealthy, found 71 percent of voters who backed Trump said cutting Medicaid would be unacceptable. Voters overall were even more opposed to it, with 82 percent saying so.
Six in 10 Trump voters also said cutting food and nutrition programs would be unacceptable.
Medicaid has increasingly become a hot topic on Capitol Hill as the GOP seeks to advance its budget proposal to pass Trump’s legislative agenda.
The House Rules Committee voted along party lines Monday to advance the budget resolution, allowing it to move to the floor for debate and a vote.
The resolution would direct the House Energy and Commerce Committee to find at least $880 billion in budget cuts, raising concerns among Democrats and moderate Republicans that it could mean cuts to Medicaid, which provides health care coverage to more than 70 million people, most of them poor and half of them children.
The committee has jurisdiction over the program, and many lawmakers believe making cuts to it, along with food assistance programs, is the only way to reduce spending.
This has forced House GOP leadership to work to win over the more moderate members of the conference who have expressed concern about the possibility.
Continued
| |
House Republicans representing large shares of Medicaid, SNAP beneficiaries face tough budget test
By Melanie Zanona, Sahil Kapur, and Ben Kamisa, NBCNews, February 21, 2025
The House’s sweeping budget plan to advance President Donald Trump’s agenda could result in steep cuts to Medicaid and food stamps, putting a key group of Republicans in a politically difficult position ahead of a potential vote next week in the narrowly divided chamber.
There are a handful of House Republicans who represent parts of the country where sizable shares of the populations receive government assistance from Medicaid and the Supplemental Nutrition Assistance Program, according to an NBC News analysis of the most recently available Census Bureau data.
The lawmakers from the 10 GOP-held districts with the highest percentages of Medicaid or SNAP beneficiaries span the ideological and geographical spectrum. They include members from deep-red districts, such as Speaker Mike Johnson of Louisiana and veteran Rep. Hal Rogers of Kentucky, as well as those in competitive battlegrounds, such as Reps. David Valadao of California, Rob Bresnahan of Pennsylvania and Monica De La Cruz of Texas.
While Democrats represent more districts with the largest portions of adults receiving federal assistance, the prevalence of constituents who are dependent on anti-poverty programs in GOP-held seats could test Republicans who are on the hunt for steep spending cuts and under pressure to implement Trump’s agenda. And it underscores why the issue has become such a sticking point in the budget talks.
“There’s a little bit of frustration among those of us who do have large Medicaid populations that we have not been engaged [by leadership] as much as some of the members of the Freedom Caucus in this process,” Rep. Nicole Malliotakis, R-N.Y., told NBC News.
“And therefore, we are undecided on how we’re going to be voting,” she continued, referencing the GOP holdouts with concerns about Medicaid.
Continued
| |
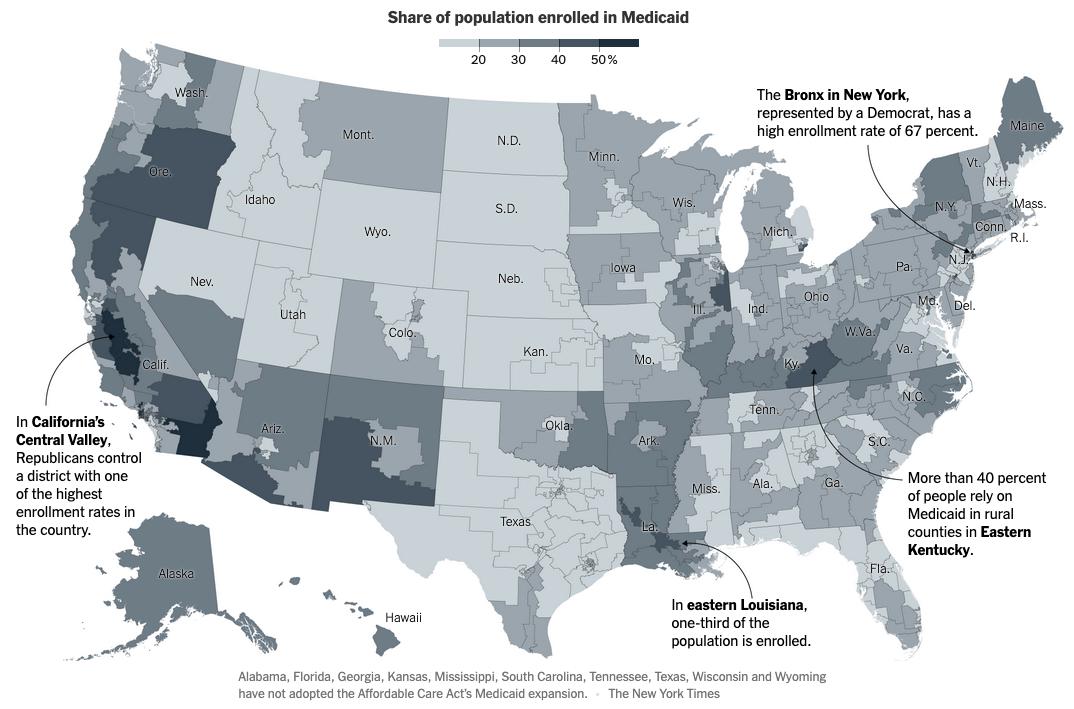
More Than 70 Million Americans Are on Medicaid. This Is Where They Live.
By Sarah Kliff and Martín González Gómez, The New York Times, February 27, 2025
In the stretch of rural Kentucky that borders West Virginia, voters reliably send Republicans to Congress. Representative Hal Rogers, who represents the area, did not even face a Democratic challenger in 2024. More than 40 percent of the population there relies on Medicaid, the public health insurance plan for low-income Americans.
In eastern Louisiana, where Representative Julia Letlow, a Republican, was elected in 2024 by a wide margin, about one-third of the population is enrolled in the program.
| |
And in California’s Central Valley, Republicans control a district where two-thirds of the population is on Medicaid, one of the highest rates in the nation, according to an analysis of federal enrollment data by the Center on Budget and Policy Priorities, a liberal think tank.
Some of those places could bear the brunt of steep Medicaid cuts that are expected to be central to Republicans’ budget plans. The budget passed on Tuesday night by House Republicans directs Energy and Commerce, the committee that oversees Medicaid, to cut spending by $880 billion over the next decade, which would amount to an 11 percent reduction in the program’s planned spending.
Continued
|
Shortsighted Medicaid Cuts Will Endanger the Lives and Jobs of Millions
Article by Staff Contributors, PHI, February 19, 2025
PHI is an organization representing the National Direct Care Workforce
As part of a broader agenda to slash federal funding for critical health and social service programs, the 119th Congress is considering deep and lasting cuts to Medicaid. If enacted, these cuts would endanger millions of older adults, people with disabilities, and people with serious illnesses who rely on the program, including but not limited to those who rely on Medicaid for their long-term care. Cuts would also devastate the direct care workers who provide those services—with cascading negative effects on quality of care, on the lives and livelihoods of family caregivers, and on our nation’s economy.
Medicaid is Fundamental to Long-term Care
Medicaid is the primary payer for long-term services and supports in our country, since Medicare and private health insurance do not normally provide long-term care coverage. Medicaid covers home and community-based care for 7.8 million Americans, while also covering care for 1.5 million in nursing homes across the country (that is, six out of every ten nursing home residents). Despite the program’s vast reach, many people do not realize that their own (or a loved one’s) care is provided by Medicaid, since the program goes by different names in different states (like TennCare or Medi-Cal) and can be operated through private insurance companies (like UnitedHealth or Centene).
Medicaid is a critically needed social safety net program. Before Medicaid will begin paying for long-term care services, applicants must demonstrate that they do not have other insurance that would pay for care, that they do not have sufficient income or assets, and that they have a clinical need for help with activities of daily living. Nationally, older adult and disabled beneficiaries make up 21 percent of Medicaid recipients but account for 52 percent of spending due to often-complex care needs; accordingly, cuts to Medicaid will have a disproportionate impact on services and supports for the Americans who need them most.
Medicaid is Fundamental to the Quality of Direct Care Jobs
More than five million direct care workers—personal care aides, home health aides, and nursing assistants—provide essential daily care and support across care settings. Medicaid is the largest payer for all long-term services and supports (LTSS) in the U.S., accounting for more than 44% of all LTSS expenditures. Direct care workers assist individuals with activities of daily living, such as bathing, dressing, and eating. They manage medications and monitor chronic conditions, depending on their role, and may provide support with tasks like scheduling, attending appointments, or engaging in community activities or employment. Direct care workers foster independence, help overcome social isolation, and serve as a key link between individuals receiving care, family members, and other health care and social service professionals. In many cases, they are a lifeline for clients.
Driven by an aging population that is living longer with more complex conditions, demand for direct care will continue to rise. In fact, direct care jobs represent our nation’s largest occupation with the most anticipated growth. It is estimated that this sector will add nearly 860,000 new jobs to the economy between 2022 and 2032.
Despite their importance, the jobs held by direct care workers are undervalued. As documented in PHI’s Workforce Data Center, the median wage for direct care workers is $16.72 per hour, resulting in 37 percent of the workforce living in or near poverty. Nearly half (49 percent) access public benefits in order to make ends meet, including 31 percent who rely on Medicaid for their health care coverage. Poor job quality and limited training and advancement opportunities are pushing potential and existing direct care workers into other fields that offer better pay, benefits, and career progression. As a result, employers struggle to recruit and retain workers, despite the high demand for their services.
Medicaid cuts will further magnify challenges to the quality of direct care jobs, and worsen recruitment and retention challenges. Loss of coverage for individuals will cause providers to reduce workers’ hours. Some employers may close down altogether. The destabilization of the LTSS operating landscape will make it more difficult for workers to achieve stable schedules and a livable wage. Many workers will also be at risk of losing their own Medicaid coverage, alongside other essential supports.
A shortage of workers and services will force family members to stay home from work and out of the economy to care for loved ones, with a disproportionate impact on women. People who might otherwise receive care at home may be institutionalized at an even greater expense to themselves and the government. Long-term care facilities are already facing capacity challenges and will also be directly impacted by Medicaid cuts, limiting their ability to meet additional demand for care. Ultimately, many will go without essential services and supports, driving higher costs for other health care service providers, including hospitals and emergency departments.
Continued
| |
|
February 27th is Rare Disease Day
Did you know that:
💠There are 7,000 Rare Diseases.
💠72% of them are genetic.
💠It can take 5 Years on average to diagnose.
💠95% do not have a single FDA-approved drug treatment.
Many of these rare diseases cause or may be associated with intellectual disabilities and autism.
| |
Opinions - Words from Friends | |
Adults with Disabilities Deserve to Work
By Jill Escher, The Free Press, February 26, 2025
Margo B. works diligently, sitting at her worktable at the South Valley Training Company in Sandy, Utah. Her job is to put silicone toe separators—a medical device similar to what might be used during a pedicure—into their white packaging. She repeats this process until there are no more products to be boxed. Then it’s time for her break at the soda machine. She works for four hours a day, two days a week, although she would love to work more. On another day she might load felt-tip markers into boxes, or smooth O-rings onto plumbing plugs.
For this work, she is paid 10 to 30 percent of the prevailing wage for such tasks in her state, based on her lower than standard level of productivity.
Margo, who is 31 years old, has autism and Down syndrome, which affect her coordination and fine motor skills. She would struggle to do the majority of jobs. But like most people her age, she has a deep desire to be productive and earn some extra cash. And so, since 2017, she has worked at the South Valley Training Company—a nonprofit that offers developmentally disabled adults various services, including the opportunity to work. Margo is employed under Section 14(c) of the federal Fair Labor Standards Act from 1938, a law that has long allowed certain employers—more than 90 percent of which are disability nonprofits—to pay their disabled workers less than minimum wage.
With roots in the interwar period, when Congress wished to incentivize employers to hire the blind, and later, wounded veterans, the logic of Section 14(c) is simple: Disabled people have just as much right to contribute to society via work as any American. To make this financially feasible, wages may be adjusted to reflect productivity levels. Those with disabilities who are “otherwise qualified” to perform the essentials of the job—for example, a computer coder who uses a wheelchair—ought to be fully compensated for their work. Those whose productivity is reduced by severe intellectual and developmental disorders and who might require hands-on, often intensive supervision—this is who 14(c) applies most often to today—may qualify for a subminimum wage.
As an autism advocate, I have spoken to many individuals who earn subminimum wages, and for them, the money is almost never the point. Most don’t only want to work in order to get healthcare and spending money. Their work is usually part of a broader package of benefits including on-site supervision, Social Security payments for disability, Medicaid, and housing subsidies. Rather, they’re seeking purpose and pride, and a sense of responsibility. “Her job has been a blessing,” said Margo’s mother, Anna, who declined to share her or her daughter’s last names. Although Margo uses few words, her mother tells me that she comes home from a day of work with a smile. “She has thrived so far beyond what anyone expected.”
But soon, Margo could lose her opportunity to work. That’s because federally funded disability rights organizations have been pushing for a phaseout of job programs that pay subminimum wage, arguing that they are exploitative. What’s more, advocates claim that adults with disabilities, no matter their level of impairment, should be encouraged to pursue competitive jobs that any other, nondisabled adult might have.
Continued
| |
“Inclusion” Means Exclusion for Disabled Students in Massachusetts
By John Hirschauer, City Journal, February 27, 2025
In January, the Massachusetts Department of Public Health announced plans to close the Pappas Rehabilitation Hospital for Children, a hospital-school in Canton for students with severe physical disabilities. The decision was celebrated by the state’s public health commissioner, Robbie Goldstein, who believes that many of the school’s children “actually could be better cared for, more safely cared for, more compassionately cared for at home.” But the announcement devastated students, families, and staff, who say that the 160-acre facility is the best place for children with complex medical and developmental challenges. Though public opposition has prompted Governor Maura Healey to “pause” the closure until further notice, Pappas and its students remain in jeopardy.
Founded as the Massachusetts Hospital School in 1907 and renamed in 2017, Pappas is home to some of the state’s most severely disabled students. The school’s sprawling campus hosts nurses, doctors, and specialists, providing a self-contained therapeutic environment and full suite of services. While the facility has capacity for 60 students, federal and state policies that discourage special residential placements for disabled students have reduced its census to 36. Many of these children have nowhere else to go.
Danielle D., who graduated from the then-Massachusetts Hospital School in 2015, was in crisis when she first came to the facility. Diagnosed with limb-girdle muscular dystrophy as a child and eventually confined to a wheelchair, Danielle was physically and sexually abused at home, shuttled in and out of foster care, and routinely excluded at her town’s public elementary school.
“I used to sit there on the couch [at the foster home] and watch the kids run and play, run and play, and I would cry, and I would wish I could run like them and . . . wish I could play like them,” she said. At school, “I would go to recess and I would just sit there and watch all the kids have fun. I would pray to God that my legs worked like them one day.”
Danielle’s health continued to decline, and she often missed class for one of her many specialist appointments. Her life changed after she returned to her father’s custody and was sent to a summer camp for children with muscular dystrophy on the then-Massachusetts Hospital School’s campus.
“It was one of the best weeks of my life. I was in a room for the first time with kids that looked just like me. There wasn’t any more, ‘Oh, I have to sit and watch.’ I can play with all of these kids and I can keep up with them. We’re all the same.”
Danielle’s father admitted her to MHS in 2007, ahead of fourth grade. The adjustment was challenging; she compared her bewilderment on her first night with a scene out of Monsters, Inc. But she came to view the nurses and staff as loving parents, and her classmates as companions in facing disability’s harshest challenges.
“You go to a public school, you’re bullied for being rare, you’re looked at for being different, you have to prove you’re this, or prove you’re that.” At MHS, she said, she could function as a wheelchair user “alongside kids that are going through the same thing that you’re going through.”
Pappas’s exclusive focus on disabled children made Danielle feel welcome. But to some disability-rights activists, this feature of the school is the very reason that it and other facilities like it must close. UNICEF, for example, believes that “residential special education should no longer be permissible in any education system, for any children with disabilities.” The National Council on Disability, an independent federal agency with activist commitments, lamented in a 2018 report that “many students with disabilities remain segregated in self-contained classrooms or in separate schools.” The report, titled “Segregation of Students with Disabilities,” spotlighted Massachusetts as one of the states with “the highest rates of placements in special facilities.”
Michael Poirier, a former patient and later staff member at Pappas, argued in a social media post that Massachusetts “has not wanted to be in the hospital business for years.” He believes that the state’s desire to close the facility is at least partly ideological, arguing that Commissioner Goldstein considers Pappas a “restrictive institution” and “does not believe [that] a person with a disability can be isolated in community settings.”
Massachusetts has relied on similar reasoning to close other public facilities. The state has shuttered five of its seven public institutions for people with developmental disabilities since 1992. Like Pappas’s students, many of those facilities’ residents were admitted voluntarily. And like Goldstein, proponents of those closures believe that the state has a moral obligation to remove the disabled from institutions that they or their guardians have chosen.
Continued
| |
Budget shortfall means Colorado’s young children with developmental delays will get fewer services
By Jenny Brundin, CPR News, February 27, 2025
Physical, speech and behavioral therapy for young children with developmental delays could get cut back starting as early as Monday due to a $4 million budget hole in Colorado’s Early Intervention program.
The changes would impact potentially thousands of children, especially those from low-income families who are on Medicaid.
The sudden news delivered in a letter Tuesday sent shockwaves through the community of therapists who provide services to some of the state’s most vulnerable children. Many expressed anger, sadness and frustration. Colorado’s Department of Early Childhood hasn’t officially informed families of the changes, but the news had already trickled out to many families.
The Early Intervention program, which provides early evaluation and therapeutic support, serves more than 11,000 children up to 3 years old. The $87 million program is funded through federal and state dollars and private health insurance, with 70 percent of funding from the state.
The letter stated that “emergency response measures” are necessary to balance the program’s budget because of increased referrals, federal COVID stimulus dollars running out and a decrease in the number of the program’s children who are enrolled in Medicaid.
It said the department evaluated areas “where the program is more generous than required in state or federal law.”
Therapy will be cut back to four hours a month. Families with children with high needs, for example Down Syndrome, might work with a speech pathologist, physical therapist and occupational therapist each one hour a week. Now they’d have to choose one therapy over the other or see each more sporadically. Under the changes, newly eligible children would also have to wait longer before starting therapy.
Cuts will hurt poor families the most
Providers are especially angry about a change that prevents children who are on Medicaid from receiving certain therapies.
Medicaid covers occupational therapy, speech language pathology and physical therapy. It doesn’t cover developmental intervention, social and emotional services including mental health and behavioral support, ASL interpretation and instruction, audiology support, support for the visually impaired or registered dieticians. Up until now, families have gotten those critical services through state or other funding sources.
Early Intervention officials said those families must be provided a service that is eligible for payment through Medicaid.
Read the full article here
Read a related article from Chalkbeat here
| |
Deaths of Utahns with disabilities call attention to safety in group homes
By Annie Knox and Daniella Rivera, KSL TV, February 27, 2025
Several Utahns with disabilities have died while in the care of group homes in recent years, with advocates and family members saying many of those deaths were preventable.
The KSL Investigators examined three tragedies since 2022 that have drawn attention to safety in facilities overseen by the state.
In April 2022, Chien Nguyen walked out of the Hidden Hollow Care Center in Orem and into the road, where he was hit and killed by an employee’s car. According to Utah’s Disability Law Center, Nguyen had attempted suicide a day earlier and had gone one to two weeks without his psychiatric medication that addressed suicidal ideation.
In November 2023, another untimely death occurred. Malachi Portwood, a 16-year-old boy with autism, escaped from Future Rising in Salt Lake County.
“He was an elopement risk and they knew that, and so they were supposed to have alarms in the door, so if he went out the door, they would know,” said attorney Nate Crippes with the Disability Law Center.
But the agency did not install alarms, even though Malachi had run away a week earlier, Crippes said. In the weeks before the teenager’s death, Crippes said an employee raised concerns three times to administrators at Utah’s Division for People with Disabilities, but the state failed to act.
The day of his death, Malachi crashed a van and seriously injured a motorcyclist. He was shot and killed by police trying to stop him. Now the employees who were caring for Malachi are under criminal investigation, with police saying they lied about when and how he went missing.
“What scares me the most is there’s other kids with these people,” Autumn Portwood, Malachi’s mother, told KSL.
Nguyen and Portwood’s experiences were focal points in the Disability Law Center’s complaint to federal health administrators last year, alleging the state isn’t meeting its obligations to make sure Utahns are safe in facilities with state licenses and contracts.
In a statement to KSL, a Utah Department of Health and Human Services (DHHS) spokesperson said the agency “remains committed to owning these challenges.”
“We take the health and safety of those in our licensed and certified facilities seriously,” the statement continues.
Crippes said problems remain. He told KSL that some smaller private agencies providing care to Utahns with disabilities are taking on clients who require a high level of supervision and care.
“Are they capable of providing those services? What we see in at least a few instances is, no,” Crippes said.
The budget for Malachi’s care, according to the Disability Law Center: $400,000 per year.
DHHS wouldn’t talk about specific cases. But a spokesperson told KSL they hold providers accountable when they don’t meet health and safety standards, giving out warnings and sometimes even taking away licenses.
The facility where Nguyen died lost its license and closed in June 2023, after it was criticized in a report from the Disability Law Center titled “License to Mismanage.”
The company caring for Malachi was fined $500 for the events surrounding his death before the state ended its contract last year.
Continued
| |
Developmentally disabled Missourians suffer abuse, death in state’s dysfunctional system
By Kevin Skipworth, Missouri Independent via KSMU, BFebruary 24, 2025
From 2017 through 2023, roughly 2,680 people with developmental disabilities died under the care of the state of Missouri — on average, one person every day.
After Ronald Scheer was found suffocated to death by the straps of his own wheelchair, an autopsy determined his cause of death was “hanging.”
Scheer, a man with developmental disabilities and mobility issues who used a wheelchair, was living at the state-run St. Louis Developmental Disabilities Treatment Center in St. Charles in June 2020 when one of his caretakers allegedly failed to secure all the safety belts keeping him in his wheelchair,
according to court documents in a wrongful death lawsuit filed by his legal guardian.
Then, the caretaker allegedly left Scheer alone despite the fact that his prescribed care plan required them to check in on him every 30 minutes and reposition him every two hours. During that time, Scheer reportedly slipped down the wheelchair, his neck fell into one of the straps and he suffocated.
Scheer’s caretakers were not held responsible for his death because a court ruled that, as public employees, they were immune from civil suits regarding negligence on the job.
But Scheer is not the only Missourian with disabilities whose death raised troubling questions.
A review of state records, court documents and department policies, as well as interviews with frontline employees working in the state, reveal a dysfunctional developmental disability system riddled of accusations of abuse, neglect, and in some cases, concerning deaths.
From 2017 through 2023, 74 people with developmental disabilities died in some sort of accident while in state care, according to state records obtained by the River City Journalism Fund. Additionally, nine homicides and seven suicides occurred amongst this population during that time, according to the records. Another 2,200 died of natural causes and 392 had an “undetermined” cause of death.
In total, from 2017 through 2023, 2,682 people with developmental disabilities died under the care of the state of Missouri — on average, one person every day.
Lisa Goodman, a 57-year-old Warrensburg woman with developmental disabilities, is another one of those people. Two months after moving into a Kansas City group home, she choked on a hot dog given to her by her caretakers and died.
Goodman’s group home was run by an agency called the Center for Developmentally Disabled. Her disabilities meant she required a special diet with non-solid food so she wouldn’t choke.
Yet on this day in July 2019, her caretakers, who’d been briefed on her diet, gave her a hot dog. At the time she choked and died, the caretakers had stepped outside, despite the fact that her prescribed care plan required a caretaker to supervise her while she ate, according to multiple employees who worked with Goodman or had direct knowledge of the situation but asked to remain anonymous out of fear of retribution from their superiors.
An investigative report provided by the Jackson County Medical Examiner’s Office confirms that Goodman died from asphyxia due to choking on July 27, 2019.
Continued
| |
North Carolina - Medicaid is critical for people with intellectual and developmental disabilities
By Lisa Poteat, The Carolina Journal, February 26, 2025
Medicaid is a joint federal and state program that provides health insurance and access to long-term care to more than 2.6 million people in North Carolina, including North Carolinians with disabilities.
In North Carolina, there are an estimated 200,000 people living with an intellectual or developmental disability (IDD). People with IDD represent an array of conditions, including but not limited to, autism, Down syndrome, cerebral palsy, Williams syndrome, and Fragile X syndrome.
Most people living with IDD rely on Medicaid, as it is the primary health insurance for people with disabilities. Medicaid provides the means for home and community-based services (HCBS), direct support professionals (DSP), prescriptions, medical equipment, and assistive technology. HCBS includes day programs outside of the home, employment training programs, respite for caregivers, and educational activities that include learning how to create a budget.
The Arc of North Carolina is a statewide organization providing supports and services to over 5,000 people with IDD. Our staff have numerous success stories, not only about the people with IDD they serve, but their families as well.
The US House Budget Committee recently proposed, on Page 30 of their budget resolution, a per capita cap for Medicaid for each state. These caps would most likely not get North Carolina the funding needed for all Medicaid recipients and programs.
Medicaid is key to people with IDD living productive lives in the community of their choice. A loss of funding to this program would not only upend the lives of people with IDD and their families, but it would also harm North Carolina’s economy.
Medicaid allows people with IDD to live healthier and more fulfilling lives. It helps to support several facets of our state’s economy. Cuts to the the Medicaid programs they rely on would create chaos for people with IDD and their families, as well as the staff providing those necessary supports, and lead to increased unmet needs. We need improvements to be made to the Medicaid program, not cuts.
Read the full article here
| |
Montana - Billings legislator sponsors Alan's Law to make group homes safer
By David Jay, KTVQ, February 27, 2025
A bill in the Montana Legislature would bring an enhanced penalty for an offense against a vulnerable person at a caregiver facility.
The motivation for Senate Bill 296 came from an incident in Billings about a year ago, and if passed it would be called Alan's Law.
Alan Wright was beaten by a group home worker last February.
"There are a subpopulation of people that they enjoy hurting people," said Calvin Calton, Residential Support Services (RSS) executive director. "They are career predators."
Calton says RSS closed the home where the homicide happened.
"The person who died in our services, he was not only nonverbal, he had the IQ of about a 2-year-old," Calton said. "And he was non-verbal to the extent he couldn't cry for help."
Dante Garriot, who was 19 at the time, will soon go to trial for deliberate homicide in the death of Wright, who was 37.
Calton says background checks do not always reveal past offenses.
That would change if SB 296 becomes law.
"Without this law, someone could abuse someone and go to court, plead down as a misdemeanor, be released, and then they go working in another location because there's no record, no felony record," said state Sen. Mike Yakawich, R-Billings.
Continued
| |
South Carolina - Bill that aims to improve services for people who ‘fall through the cracks’ advances in SC Senate
By Shaun Chornobroff, South Carolina Daily Gazette, February 21, 2025
A bill merging a trio of agencies in South Carolina’s notoriously fractured public health system advanced Thursday to the Senate floor, less than a month after Gov. Henry McMaster publicly asked legislators to “fix this.”
The bill creates the Department of Behavioral Health and Developmental Disabilities, which combines separate agencies that oversee services for people with disabilities, mental health issues, and addictions to drugs or alcohol.
People who need assistance often need services from a combination of those agencies, said Sen. Tom Davis, one of the bill’s co-sponsors.
“Those with substance abuse problems sometimes have mental disorders. Some with mental disorders also have disabilities,” the Beaufort Republican told the SC Daily Gazette. “This is a way to better deliver those services to those populations.”
He called it a “scaled down” version of last year’s effort to merge six public health agencies, which the ultra-conservative House Freedom Caucus killed with a procedural maneuver as the clock ran out on the session.
Last month, Forbes Advisor ranked South Carolina eighth-worst nationwide in mental health care. According to the report, the Palmetto State has the nation’s highest percentage of youth with depression not receiving services, and the seventh-highest percentage of adults not receiving mental health care because they can’t afford it.
The state’s own consultant painted an even grimmer picture in a report that concluded “South Carolina is the most fragmented structure for health and human services delivery in the country.”
That’s why McMaster again used the governor’s bully pulpit last month to call for “immediate changes” at the Department of Mental Health and the Department of Disabilities and Special Needs. Both are governed by a board of commissioners “who are accountable to no one,” he said during his Jan. 29 State of the State address.
The state’s fragmented system “causes unnecessary suffering,” he said.
“Our people with physical disabilities, special needs and mental health issues seeking assistance must navigate through a confusing landscape of offices, agencies, and officials as they seek help for a loved one or dependent,” McMaster said.
“They fall through the cracks of a system that does not coordinate, communicate or collaborate,” he continued. “We must fix this.”
Continued
| |
|
Please share this offer with your loved one's
Direct Support Professionals!
VOR ❤️s OUR
DIRECT SUPPORT PROFESSIONALS!
Our loved ones' caregivers are essential to their health, safety, and happiness.
In appreciation of their good work and kind hearts, VOR offers free digital memberships to any DSP who would like to receive our newsletter.
We encourage our members to speak with their loved ones' caregivers to extend this offer of our gratitude.
If you are a Direct Support Professional interested in receiving our newsletter and e-content, please write us at
info@vor.net
with your name, email address, and the name of the facility at which you work. Please include the name of the VOR member who told you of this offer.
| |
|
What's Happening In Your Community?
Is there an issue in your loved one's home that you need help with?
Do you have information or a news story you would like to share?
Is there legislation in your state house that needs attention?
Contact us at info@vor.net
| |
|
So far this year, 2,934 bills have been introduced in the 119th Congress.
As yet, no text or summaries have yet appeared on the congressional website, so we cannot say if we support or oppose the bills.
One bill, however, does look promising. Although no text or summary is yet available, it does have bipartisan support among the 28 senators who have cosponsored the bill.:
S.752 - Chuck Grassley - (R-IA)
A bill to amend title XIX of the Social Security Act to streamline enrollment under the Medicaid program of certain providers across State lines.
Please stay tuned.
| |
836 South Arlington Heights Road #351
Elk Grove Village, IL 60007
Toll Free: 877-399-4867 Fax: 877-866-8377
| |
FACEBOOK: /VOR ----- TWITTER: @VOR_NET ----- YouTube
| | | | |