|
VOR's Weekly News Update
VOR is a national non-profit organization
run by families of people with I/DD and autism
for families of people with I/DD and autism.
| | |
First, the good news
I received a telephone call this morning from two people at the Department of Labor, Wage and Hour Division, Office of Disability Employment Policy (ODEP), informing me that the Wage and Hour Division has rescinded the Proposed Rule submitted by the Biden Administration in December, 2024 that ordered the phasing out of sheltered workshops and compensatory wages under Section 14(c) or the Fair Labor Standards Act.
They thanked me and asked that I thank VOR's families for their support on this effort.
We should all thank the leadership of the Coalition for the Preservation of Employment Choice, who really took the lead on this matter. So big thanks to Kit, Colleen, Craig, Melinda, Victoria, and the other hundred and twenty-five people who helped bring this about.
For a copy of the notice that will appear in the Federal Register,
please click here
For a copy of VOR's response to ODEP,
please click here
--------------------------------------------------
Now, the bad news
The House of Representatives just passed the "One Big Beautiful Bill", as amended by the United States Senate. The bill passed strictly along party lines.
The new bill is going to cut
ONE TRILLION DOLLARS
from Medicaid over the next ten years.
$1,000,000,000,000.00
While Intermediate Care Facilities (ICFs) and Skilled Nursing Facilities (SNFs) are said to be protected from these cuts, most VOR families are concerned that the cuts will trickle down one way or another. Home- and Community-Based Services (HCBS) are very much at risk from these cuts.
We are also concerned because, over the past decades, many VOR families have chosen to move, or been forced to move, their loved ones with I/DD and autism out of ICFs and into HCBS settings.
We are deeply concerned that some of our loved ones and some of our families are likely to lose the services they rely upon. We believe that this bill will bring harm to members of the community of people with I/DD and autism, cause some of the providers and hospitals that we rely on to close or cut back on services, further impact the shortage of Direct Support Professionals, and impose an even heavier burden upon family caregivers.
The final text of the Senate bill may be downloaded here.
A one-page synopsis of the bill may be downloaded here.
-------------------------------------------------
And now, a request
In the past months, we have tried to prevent cuts to Medicaid in the reconciliation bill. Our efforts have included:
- Written over 50 (snail mail) letters to the Governors of every state and territory showing how these cuts will impact their budgets and their ability to serve our community.
- Sent emails to every State Director of Developmental Disability Services, asking them to coordinate with their governors in opposing these cuts.
- Rallied on Capitol Hill and presented VOR's position paper opposing Medicaid cuts to every office in the House and Senate.
- Sent emails to the staffers on the House Energy and Commerce Committee, the House Appropriations Committee, The Senate Finance Committee, The Senate Aging Committee, and the Senate HELP Committee, outlining our concerns.
- Sent further rounds of emails to every office of the Senate Republicans working on the reconciliation bill.
- Sent another round of emails to a list of "on the fence" Republicans in the House earlier this week.
- Coordinated with other like-minded groups in trying to halt these drastic cuts that would harm our families
We will continue to work to protect our loved ones with I/DD and autism, and to protect our families. Much of the above information is available on our website at www.vor.net
We hope that our members agree with our efforts on this matter. As always, VOR tries to avoid partisan politics, adhering to our stated mission of advocating for high quality care and human rights for all people with I/DD and autism.
We hope, too, that our members will help us in our mission by donating to VOR here.
| |
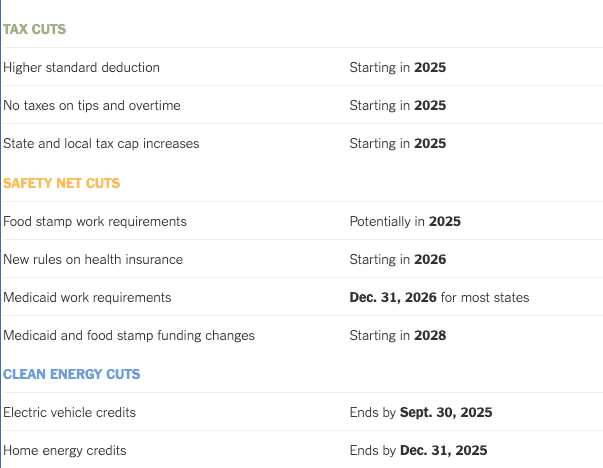
Tax Cuts Now, Benefit Cuts Later: The Timeline in the Republican Megabill
Republicans deferred some of their most painful spending cuts until after the midterm elections.
By Tony Romm, Andrew Duehren, Margot Sanger-Katz, Brad Plumer and Daniel Wood,
The New York Times, July 2, 2025
At the core of Republicans’ sprawling domestic policy package is an important political calculation. It provides its most generous tax breaks early on and reserves some of its most painful benefit cuts until after the 2026 midterm elections.
The result is a bill that, if it becomes law, may generate bigger refunds for some taxpayers when they file their returns next spring, even as a series of significant changes to Medicaid and other aid programs loom as a future threat to the finances of poorer families.
| | |
For President Trump, the staggered timelines underscore the political risks in his signature legislation, which passed the Senate on Tuesday and now awaits a final vote in the House. To pay for the tax policies, which confer their greatest benefits on the wealthy, Republican lawmakers have looked to slash programs that are both popular and widely used, discomfiting even some within their own ranks.
The savings from the safety net cuts still are not enough to offset an expensive package of tax breaks that is projected to add more than $3 trillion to the federal debt by 2034.
Continued
| |
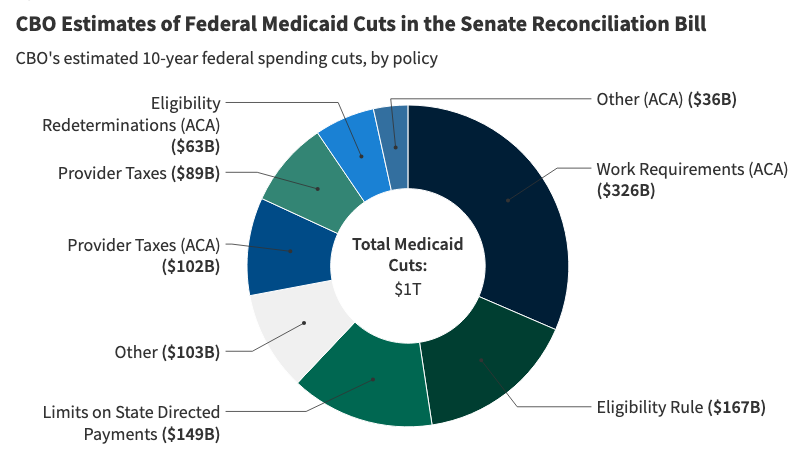
Allocating CBO’s Estimates of Federal Medicaid Spending Reductions Across the States: Senate Reconciliation Bill
By Rhiannon Euhus, Elizabeth Williams, Alice Burns, and Robin Rudowitz, KFF, July 1, 2025
The Senate passed their version of the reconciliation bill on July 1, which differs from the version that passed the House on May 22. The Congressional Budget Office’s (CBO) latest cost estimate, which corresponds to the Senate Budget Committee’s version of the bill, shows that the bill would reduce federal Medicaid spending by $1 trillion and increase the number of uninsured people by 11.8 million. Building on prior KFF analysis of the House-passed reconciliation bill, this analysis allocates CBO’s federal spending reductions in the Senate reconciliation bill across the states. The Medicaid reconciliation provisions are numerous and complicated, but the majority of federal savings stem from work requirements for the expansion group, limiting states’ ability to raise the state share of Medicaid revenues through provider taxes, increasing barriers to enrolling in and renewing Medicaid coverage, and restricting state-directed payments to hospitals, nursing facilities, and other providers.
CBO has not published updated estimates of the number of people who would lose Medicaid under the Senate’s reconciliation bill, so this analysis does not include updated enrollment estimates like those included in KFF’s analysis of the House-passed reconciliation bill. CBO’s most recent estimate of Medicaid enrollment loss from an earlier version of the House reconciliation bill was 10.3 million people in 2034, which was associated with a $625 billion decrease in Medicaid spending (reflecting preliminary estimates prepared for the House Committee on Energy and Commerce). Given the Medicaid spending reductions are considerably larger, more than 10.3 million people are likely to lose Medicaid from the Senate bill.
This analysis does not predict how states will respond to federal policy changes, and anticipating how states will respond to Medicaid changes is a major source of uncertainty in CBO’s cost estimates. Instead of making state-by-state predictions, CBO generates a national figure by estimating the percent of the affected population that lives in states with different anticipated types of policy responses. For example, different states might choose to implement a work requirement with reporting requirements that are easier or harder to comply with. In estimating the costs of the legislation, CBO assumes that in aggregate, states would replace half of reduced federal funds with their own resources in response to provisions that reduce the resources available to states, such as limits on provider taxes. For provisions that reduce enrollment but don’t affect the division of costs between the federal and state governments, such as work requirements, CBO estimates that the federal and state Medicaid spending would go down. However, those assumptions reflect states’ responses as a whole and are likely to vary and may not apply in all states.
| |
Why a G.O.P. Medicaid Requirement Could Set States Up for Failure
By Margot Sanger-Katz and Saraf Kliff, The New York Times, June 28, 2025
The strict Medicaid work requirement at the center of the Republicans’ major policy bill wouldn’t just require millions of poor Americans to prove they are employed to sign up for health insurance. It would also require dozens of states to quickly build expensive and complex software systems to measure and track who is eligible.
This new responsibility for states, whose existing Medicaid computer systems are often outdated, would be accompanied by reduced federal funding through other changes in the bill. The result, according to state officials, software developers and policy experts, could be major failures in state systems for enrolling people in Medicaid.
“That’s how Healthcare.gov happens,” said Julie Brinn Siegel, a former top Biden administration budget official, referring to the Obama administration’s botched launch
Ms. Siegel and others familiar with Medicaid systems envision problems like websites that don’t load or incorrectly tell applicants they are not eligible. And Medicaid workers may be overwhelmed as they try to run call centers and process applications. The fallout could mean eligible Americans will have their coverage dropped.
Current and former state officials fear the issues could spill outside the population of working-age adults the work requirement is designed for, causing delays and errors for children, parents and Medicaid beneficiaries with disabilities.
“The worry is the consequences will fall really to the people who rely on the program, and they’ll lose health care coverage because we didn’t have enough time to have the systems ready and for us to do it right,” said Jay Ludlam, North Carolina’s Medicaid director.
Read the full article here
| |
GOP governors stay silent amid plans to slash Medicaid spending in their states
By Phil Galewitz, Shots - NPR Health News July 3, 2025
The last time a Republican-controlled Congress and President Donald Trump moved to slash Medicaid spending, in 2017, a key political force stood in their way: GOP governors.
Now, as Congress steamrolls toward passing historic Medicaid cuts of about $1 trillion over 10 years through Trump's tax and spending legislation, red state governors are saying little publicly about what it does to health care — even as they face reductions that will punch multibillion-dollar holes in their states' budgets.
Medicaid, a program jointly run by states and the federal government, covers more than 70 million low-income or disabled people, including nearly half of the nation's children. Republicans say the $900 billion-a-year program was allowed to grow too large under Democrats Barack Obama and Joe Biden by adding nondisabled adults they say don't deserve government assistance, and they have long sought to scale it back.
Some of the biggest health cuts in the legislation Trump calls the "One Big Beautiful Bill" are achieved through new policies that would reduce enrollment by imposing more paperwork demands on enrollees, including a requirement that many prove they're working. Those policies would affect only states that expanded Medicaid to more low-income people under the Affordable Care Act.
Nineteen of those states are led by Republican governors. Their silence on the bill's health measures is giving political cover to GOP lawmakers from their states as they seek to cut Medicaid coverage for millions of people who gained it within the last decade.
Continued
| | |
The White House released its own statement earlier this week, to clarify the Myths vs. Facts of the One Big Beautiful Bill. Below are excerpts from the press release.
Myth vs. Fact: The One Big Beautiful Bill
By President Donald J. Trump, The White House, June 29, 2025
MYTH: The One Big Beautiful Bill is “just a tax break for billionaires.”
FACT: The One Big Beautiful Bill delivers the largest middle- and working-class tax cut in U.S. history. The President’s legislation will put more than $10,000 a year back in the pockets of typical hardworking families. This is the most pro-growth, pro-worker, pro-family legislation ever crafted.
MYTH: The One Big Beautiful Bill “takes from the poor to give to the rich.”
FACT: Low-income workers stand to receive the largest percentage reduction in their tax liability. The One Big Beautiful Bill delivers the largest tax cut in history for working-and-middle class Americans.
MYTH: The One Big Beautiful Bill “kicks American families off Medicaid.”
FACT: As the President has said numerous times, there will be no cuts to Medicaid. The One Big Beautiful Bill protects and strengthens Medicaid for those who rely on it—pregnant women, children, seniors, people with disabilities, and low-income families—while eliminating waste, fraud, and abuse. The One Big Beautiful Bill removes illegal aliens, enforces work requirements, and protects Medicaid for the truly vulnerable.
MYTH: The One Big Beautiful Bill “cuts Medicare.”
FACT: Medicare has not been touched in this bill— absolutely nothing in the bill reduces spending on Medicare benefits. This legislation does not make a single cut to welfare programs—it safeguards and protects these programs for all eligible Americans.
MYTH: The One Big Beautiful Bill “will close rural hospitals.”
FACT: Rural hospitals comprise just 7% of all hospital spending on Medicaid, illustrating that they have not benefited from the massive increase in waste, fraud, and abuse under the Biden administration. By strengthening Medicaid, we are making more resources available for vulnerable populations and safety net providers, like rural hospitals. We are expanding rural hospital protection, providing targeted funds for rural care, and giving states flexibility to support local providers.
MYTH: “People will literally die” from the One Big Beautiful Bill — “and millions will be kicked off their healthcare.”
FACT: This is one of the most egregious, deranged attacks from the Left peddling fear over the facts. The One Big Beautiful Bill protects eligible Americans on federal welfare – including Medicaid. By strengthening the integrity of Medicaid by eliminating waste, fraud, aprnd abuse, its resources can be refocused on providing better care for those whom the program was designed to serve: pregnant women, children, people with disabilities, low-income seniors, and other vulnerable low-income families.
MYTH: The One Big Beautiful Bill “will hurt people with disabilities.”
FACT: The One Big Beautiful Bill protects and strengthens Medicaid for Americans with disabilities. Rest assured, those with disabilities receiving Medicaid will receive no loss or change in coverage.
Read President Trump's full statement here
| |
Louisiana - Mike Johnson Warned By "Every Major Health System in Louisiana" To Vote Against Senate GOP Bill
By Lucy Strathmore, NewsBreak, June 30, 2025
| | | |
The CEOs of “every major health system in Louisiana” — Allegiance Health Management, LCMC Health, FMOL Health, La. Rural Hospital Coalition, Ochsner Health, Woman’s Hospital, and Louisiana Hospital Association — co-wrote a letter to oppose the current Senate version of President Trump’s domestic policy bill which proposes massive cuts to Medicaid.
The letter was sent to three Republican lawmakers representing Louisiana: House Speaker Mike Johnson (R-LA), Majority Leader Steve Scalise (R-LA) and Senator Bill Cassidy (R-LA), a physician who has also raised concerns about the cuts.
The healthcare leaders wrote of the bill: “These cuts would be historic in their devastation and warrant our shared advocacy to protect our patients and the care we provide them at our hospitals and clinics.”
“Cuts of the magnitude currently under discussion would adversely impact our collective ability to provide care, train the next generation of physicians, employ tens of thousands of people, and it would stifle the billions in economic impact we generate each year,” the group says in its letter.
“The impact of provisions in the United States Senate’s version of the One Big Beautiful Bill Act
reflects an estimated annual loss of more than $4 billion in total Medicaid funding for Louisiana healthcare providers.”
The letter ended: “We take no pleasure in having to speculate about the impact of these cuts. However, in light of the cuts being proposed, we must have honest conversations together, and with you – the communities we serve. Louisiana and our healthcare delivery system are at a crossroads. We face the largest cut to healthcare in our state’s history. Will our leaders in Washington choose to protect the health of our people, hospitals and economy? We are counting on them to do so.”
Conntinued
| |
Missouri - To keep Medicaid, a mom caring for her disabled adult son may soon need to prove she works
By Bram Sable-Smith, KFF Health News, June 30, 2025
Four years before Kimberly Gallagher enrolled in Medicaid herself, the public health insurance program’s rules prompted her to make an excruciating choice — to give up guardianship of her son so she could work as his caregiver.
Now, another proposed twist in the rules could mean that, even though Missouri pays her to do that work, she might still have to prove to the state that she’s not unemployed.
| |
The Kansas City, Missouri, resident has cared for her disabled son, Daniel, for all 31 years of his life. A rare genetic condition called Prader-Willi syndrome, in addition to autism, left him with an intellectual disability; a constant, excessive hunger; and an inability to speak. His needs left Gallagher, an elementary school teacher by training, with little opportunity to work outside her home.
As congressional Republicans consider slashing about $1 trillion in federal Medicaid spending, Gallagher is among the 18.5 million Americans who could be required to prove that they work enough to keep their health insurance.
Budget bills in the House and Senate would require 80 hours of work or community service a month for adults who are insured through the Affordable Care Act’s Medicaid expansion program, which has allowed states to extend Medicaid coverage to more adults with low incomes. Forty states, plus Washington, D.C., have expanded their programs, additions that now cover about 20 million Americans, including Gallagher.
The Medicaid program that pays for in-home care for Daniel and 8,000 other Missourians with disabilities allows family members to be compensated for caregiving, but only if they’re not the legal guardian of the person they care for. So, Gallagher went to court to give up her rights to make decisions for her son and transfer authority to her parents.
“I think it’s appalling that it’s required, but it was necessary,” she said. “There was no way I could work outside of taking care of Daniel.”
Republicans have touted Medicaid work requirements both as a way to reduce federal spending on the program and as a moral imperative for Americans.
“Go out there. Do entry-level jobs. Get into the workforce. Prove that you matter. Get agency into your own life,” Mehmet Oz, administrator of the Centers for Medicare & Medicaid Services, said in a recent interview on Fox Business.
Read the full article here
| |
North Carolina - The disabled teen stuck in a hospital for six years finally gets her own home
By Joseph Shapiro, NPR - All Things Considered, July 1, 2025
Alexis Ratcliff is 19 and she's lived, since she was 13, in a hospital in North Carolina. This week, the disabled woman moved to her own apartment. When she saw the spacious, renovated place for the first time, she celebrated. "Oh, it's beautiful," she said, her voice quiet and awed, as she maneuvered her power wheelchair down the wide and newly built wood ramp.
The Trump administration celebrated, too, and put out a press release to mark its role in helping the state get Ratcliff home. But the release from the U.S. Department of Health and Human Services left out one detail: The Trump administration, in its budget request for the next fiscal year, zeroed out the money for the program that helped Ratcliff move.
| | |
NPR described Ratcliff's plight in a story last year. She was a baby when a car accident left her with significant disabilities. She's quadriplegic and uses a power wheelchair, which she controls by moving a joystick with her chin. She needs a ventilator — 24 hours a day — to breathe.
Her grandfather became her primary caregiver. But when he developed serious health problems when Alexis was 13, there was no longer a home or people to care for her.
She moved into a hospital in Winston-Salem, N.C., for what was supposed to be a short stay.
It lasted for six years.
When Alexis turned 18 in 2023, the hospital — Atrium Health Wake Forest Baptist — tried to get her to leave and sued her for trespass. Officials said they needed the space in the intensive care unit for other patients, and wanted Alexis to agree to move to a distant nursing home in another state.
She refused. She wanted to stay near her family and friends, and to accept a scholarship from a local college.
Plus, leaving North Carolina would mean she might never return because there was no guarantee she could get back onto the state's Medicaid program.
Over the years, Ratcliff got excellent care at the hospital, which kept the quadriplegic teen free of bed sores and respiratory illnesses. Nurses and staff at the hospital became her friends and advocates, throwing parties on her birthday and when she graduated, with honors, from high school.
But things soured once the hospital pressured Ratcliff to move. Officials at the hospital took her wheelchair, her lawyers say, and told her that if she went outside she would not be allowed back through the doors of the hospital. After the NPR story, the hospital dropped its lawsuit against the teen.
Asked about Ratcliff leaving the hospital, hospital officials released a statement saying they could not comment on "specific cases due to patient confidentiality." And added: "Providing care in the most appropriate setting — especially for patients with extended or complex needs — is central to our mission. Hospitals, by design, are not intended to serve as long-term residences for patients over multiple years."
Read the full article here
| |
Tennessee - One Nashville Family’s Struggle with Autism — and the Breakthrough That Politics Could Stop Cold
By Jared Sullivan, The Nashville Banner, July 1, 2025
The GOP’s ‘big beautiful bill’ and federal grant cuts have already rocked research institutes — this is how one Vanderbilt psychiatrist and one Nashville family are already contending with the country’s new scientific reality
| | |
Wendy Stotsenburg didn’t know what was happening to her son. Her second-born, Lukas, had been diagnosed with profound autism when he was 10 years old. He could neither read nor write nor carry on a conversation. But, in the five years since his diagnosis, he had made encouraging progress. Thanks to the help of Wendy and her husband, Rod, and physicians near their home in Old Hickory, Lukas could eat with utensils and say simple phrases, such as “juice box, please.” And, most important, he was happy. He loved school and watching “Sesame Street.” In 2019, Wendy had to leave her corporate marketing job after she was unable to find an after-school caretaker for Lukas. Still, despite such occasional headaches, their family had fallen into a comfortable rhythm.
Then, in March of 2020, the COVID-19 pandemic forced Lukas’s school to go remote. Stuck at home, he spent hours pacing between the kitchen and the dining room. And when he wasn’t pacing, he often wore a blank look. He urinated on himself. He held his right hand in an odd, crooked position. He lost the ability to drink from cups or water bottles. He stopped using forks or spoons, and he ate almost nothing.
Whenever Wendy set a bowl of rice on the table, he would stare at it, take a handful of grains, and watch as they fell through his fingers.
The syndrome no one looked for
About a quarter of children with autism have profound autism, like Lukas. These children have significant intellectual disabilities, with IQs about half that of their peers, and they require constant care. Lukas had suffered setbacks in the past, but neither parent could understand why he had regressed so severely, so suddenly. Was it because of his school closure, or something else?
As a year of quarantine ticked by, Lukas’s condition grew dire. Seized by unprovoked rage, he would throw chairs across the living room and chase his older sister through their home, forcing her to barricade herself in a bedroom. Once, as Wendy drove, he grabbed her ponytail and tried to drag her into the backseat. What bothered Wendy most, though, was when Lukas stopped talking. She had always felt fortunate that, though Lukas couldn’t hold a conversation, at least he could speak — many profoundly autistic children cannot — and she feared she might never hear his voice again.
One night in September of 2021, Wendy, desperate for answers, searched the internet for anything she could find about autistic teenagers who paced. Lukas’s neurologist had attributed his behavior to autism, nothing more. But, in Wendy’s view, his symptoms were all too dramatic, all too confounding, for that explanation. As she read, she happened upon another possibility. “Have you considered autism-related Catatonia?” she wrote to the neurologist the next morning. “The description of this sounds like Lukas.”
Catatonia, a neuropsychiatric syndrome, was first described in 1874 by the German psychiatrist Karl Kahlbaum. Then, as now, catatonia’s defining characteristic was stupor. When catatonic, people often become immobile and lose the ability to speak, as if they’re in a living slumber. The lights are on but nobody’s home, as one doctor put it to me. Other patients, like Lukas, move excessively but nonetheless regress. In any case, doctors have no clear idea what causes catatonia, only that it’s triggered by myriad factors: stroke, infections, poisoning, neurodevelopmental disorders, even fear.
The syndrome is rare, affecting fewer than 30 people per 100,000. But in recent years, doctors, who have historically understudied catatonia, have recognized its high occurrence among people with autism. Studies estimate that the prevalence ranges from 12 to 17 percent among all autistic individuals, while the rate is thought to run closer to 35 percent among autistic children. But even that figure could be low, since clinicians can easily mistake catatonia for sleepiness or irritability in young patients.
“Catatonia is being recognized as one of the most important problems in psychiatry and within our general hospitals across the country,” said Brian Barnett, a psychiatrist at the Cleveland Clinic. That’s because if catatonia goes untreated, it can lead to blood clots, malnutrition, pneumonia, and self-harm. The mortality rate can reach as high as 50 percent in undiagnosed cases, largely because patients stop eating.
For Wendy, reading about catatonia was revelatory — she finally had an explanation for Lukas’s baffling behavior, and maybe now his doctors could help to reverse it.
Lukas’s neurologist wrote him a prescription for Ativan, a benzodiazepine that’s commonly used to treat catatonia. Within three days, Lukas began to speak again, but his aggression didn’t abate, and he still couldn’t use the bathroom, buckle his seatbelt, or take off his clothes without help.
A stigmatized therapy, and a child in crisis
On February 18, 2022, Lukas’s aggression crescendoed. First, he lashed out at Wendy as she tried to give him medication, ripping her shirt. Then he targeted Rod as he opened mail in the kitchen. The couple attempted to coax Lukas into his bedroom, the one place he could settle himself. When he failed to calm down there, they contacted his psychiatrist, who advised them to call 911.
Once on the scene, first responders restrained Lukas, put him on a stretcher, and transported him to the children’s hospital of Vanderbilt University Medical Center.
Lukas had poor experiences at Vanderbilt in the past, and Wendy was reluctant to try it again. This time, to her relief, she and Rod met psychiatrist Joshua R. Smith. When Smith was young, one of his sisters died due to complications from a chromosomal abnormality, and her death put him on a track toward medicine. He had a deep interest in catatonia, an uncommon specialty, and, though early in his career, he had seen situations similar to Lukas’s, where a medical system had blamed a patient’s regression on autism. “But that’s not right,” Smith said.
Catatonia and profound autism have overlapping signs, like mutism and staring, but people with autism seldom regress from their baseline, or normal, condition after they turn two or three years old — that is, they don’t rapidly lose skills they’d mastered, whereas with catatonia they do, and fast. “Everything comes crashing down,” Smith explained.
At Vanderbilt, Smith adjusted Lukas’s medications, and, after four grueling days in the hospital, he calmed down enough to return home. Before the family left, Smith told Wendy and Rod that he was starting a clinic, one of the first of its kind, at Vanderbilt to study catatonia. He invited them to participate.
Wendy agreed, and began bringing Lukas for appointments. But over the next few months, his aggression didn’t wane, despite his adjusted medications. Next, Smith recommended that Lukas try electroconvulsive therapy, or ECT, the other primary therapy for catatonia.
During the procedure, a doctor places electrodes on the patient’s head, then a device sends small electrical pulses into the brain, effectively resetting it with a brief seizure. ECT was highly stigmatized in the mid-century, following a series of abuses, but the medical community has now widely accepted ECT — when administered appropriately — as an effective therapy for catatonia, along with major depression, schizophrenia, and bipolar disorder.
Still, Wendy had doubts. Did she really want us to do this to her child? Even some doctors who support ECT find it unsavory to strap down and shock patients. But for many families, the hope of recovery outweighs their misgivings. Amy Lutz, a historian of medicine at the University of Pennsylvania, estimates that her autistic son has received ECT more than 600 times over the past 15 years. “His entire quality of life hinges on the stability that ECT brings him,” she said. “There’s no doubt in my mind that without it he would be on a very restrictive, locked ward,” rather than living at home.
Wendy, hoping for a similar outcome for her son, agreed to move ahead. She drove Lukas to Vanderbilt once a week, but his aggression didn’t subside after his first treatment, or his second, or his third. ECT had to work, Wendy told herself, because Lukas had no other options.
The first sign of improvement came after nearly 50 treatments when Lukas stopped repeating a nonsensical phrase he’d been saying for months. Then he began to eat again: mashed potatoes, mac and cheese, nutrient shakes. Soon, his aggression eased. “It wasn’t a magic wand,” Wendy said of ECT. Still, his improvements were significant, lifesaving even.
What science can reverse — and what it can’t
From 2021 to 2024, Smith and some of his colleagues treated 44 other autistic patients with catatonia. Some had likely had chronic catatonia for years, and their symptoms had crystallized owing to a lack of effective treatment. A few were in critical condition from having eaten so little.
Past studies on catatonia had largely been anecdotal in nature. Smith’s team, in contrast, carefully tracked patients over three years, producing quantitative data on the efficacy of treatments, in what proved to be one of the largest clinical studies of catatonia to date. Smith first treated members of the group with various drugs. Then, if medication alone proved ineffective, he turned to ECT. Sixteen patients, including Lukas, received the treatment.
In a paper published earlier this year, Smith showed that a combination of medication and ECT measurably improved the conditions of all 45 patients, a significant finding in support of ECT’s efficacy in treating the most severe, medication-resistant cases of catatonia.
“Overall ECT has been above and beyond anything we could have possibly imagined,” said Jackie Kancir, the executive director of the National Council for Severe Autism. Kancir’s 21-year-old daughter, Jadyne, has profound autism and catatonia. She began ECT at Smith’s clinic in 2023, and because of treatment, Kancir said, “Her language is better, her balance is better, her fine motor skills are better.”
Unfortunately, Jadyne was an outlier: only 10 percent of Smith’s research group — five individuals — returned to baseline, entirely escaping catatonia’s clutches. For the other patients, including Lukas, their quality of life, though improved, remained worse than it was before catatonia set in. “Catatonia is almost like a traumatic brain injury in a way,” Smith explained. “There are long-lasting effects we don’t understand.”
The lifeline that budget cuts could snap
Wendy and Rod Stotsenburg, though grateful for Lukas’s improvements, still grapple with the fact that, now 19, he may never function as well as he once did. For Wendy, his ordeal has underscored how poorly the public health-care system is set up to aid children and adults alike who have profound autism or catatonia. Tennessee, like many conservative states, provides minimal support for disabled residents, making federal benefits essential for families. Lukas receives about $660 a month from Social Security to help cover his care. He gets health insurance through Medicaid, which provides coverage for 72 million disabled or poor Americans.
“These kids will need lifelong care,” Wendy said. “I’m going to die; my husband is going to die. Where is my son going to go?”
The GOP-controlled Congress has compounded such concerns. In May, House Republicans passed their version of a budget bill that aims to slash more than $500 billion in funding to Medicaid over the next eight years in order to pay for President Trump’s tax cuts, which stand to disproportionately benefit wealthy households. The Senate is now scrambling to pass its own version before the upcoming July 4th holiday. The proposed Medicaid cuts in its bill would leave an estimated 11.8 million people uninsured, as well as add nearly $4 trillion to the national debt over a decade.
“The threats to Medicaid have put the profound-autism community into a complete panic,” said Lutz, the historian of medicine.
Parents fear that the budget cuts, if enacted, would reduce their child’s access not only to specialized clinics like Smith’s but even to basic medical care. Kancir, who lives in Paris, Tennessee, worries that if states, which administer Medicaid for the federal government, receive reduced federal funding, they might look for savings by limiting care for high-need populations. And if that were to happen, “I don’t know what more we could lose,” she said. “The state of Tennessee can’t” — or won’t — “provide anything for us.”
Kancir was approved under Medicaid to receive in-home care for her daughter, but, because Tennessee invests relatively little in public health, she is one of more than a thousand people in the state waiting for such services, according to the latest data. Kancir and her daughter would move to another state with better public care options, but she said Smith’s clinic keeps them in Tennessee.
Federal cuts to scientific research stand to be no less consequential. President Trump’s budget proposal calls on Congress to slash $18 billion in funding — a 40% reduction — next year to the National Institutes of Health (NIH), jeopardizing grants that support research at universities and medical centers across the country. Already this month, Vanderbilt announced that it planned to terminate up to 650 staff members as part of a $300-million budget reduction — a direct consequence of federal grant cuts, both expected and already in effect. Smith, like many Vanderbilt researchers, is still trying to determine the full effect of the cuts on his clinic and department. They could be perilous.
Continued
| | |
Please share this offer with your loved one's
Direct Support Professionals!
VOR ❤️s OUR
DIRECT SUPPORT PROFESSIONALS!
Our loved ones' caregivers are essential to their health, safety, and happiness.
In appreciation of their good work and kind hearts, VOR offers free digital memberships to any DSP who would like to receive our newsletter.
We encourage our members to speak with their loved ones' caregivers to extend this offer of our gratitude.
If you are a Direct Support Professional interested in receiving our newsletter and e-content, please write us at
info@vor.net
with your name, email address, and the name of the facility at which you work. Please include the name of the VOR member who told you of this offer.
| | |
[Please click on blue link to view information about the bill]
VOR SUPPORTS:
H.R.1950 - Rep. Mark Pocan (D-WI)
To protect benefits provided under Social Security, Medicare, and any other program of benefits administered by the Social Security Administration or the Centers for Medicare and Medicaid Services.
H.R.869 - Rep. Susie Lee (D-NV)
To require full funding of part A of title I of the Elementary and Secondary Education Act of 1965 and the Individuals with Disabilities Education Act.
H.R.1509 - Rep. Lori Trahan (D-MA)
Accelerating Kids' Access to Care ActTo amend titles XIX and XXI of the Social Security Act to streamline the enrollment process for eligible out-of-state providers under Medicaid and CHIP.
S.752 - Sen. Chuck Grassley (R-IA)
Accelerating Kids' Access to Care Act - A bill to amend title XIX of the Social Security Act to streamline enrollment under the Medicaid program of certain providers across State lines.
S.779 & H.R.1735 - Sen. Alex Padilla (D-CA) & Rep. August Pfluger (R-TX)
To amend title XIX of the Public Health Service Act to provide for prevention and early intervention services under the Block Grants for Community Mental Health Services program
H.R.2491 & S.1227 - Rep Kat Cammack (R-FL) & Sen. Edward Markey (D-MA)
To require the Administrator of the Centers for Medicare & Medicaid Services and the Commissioner of Social Security to review and simplify the processes, procedures, forms, and communications for family caregivers to assist individuals in establishing eligibility for, enrolling in, and maintaining and utilizing coverage and benefits under the Medicare, Medicaid, CHIP, and Social Security programs
H.R.2598 - Rep Jared Huffman (D-CA)
To amend part B of the Individuals with Disabilities Education Act to provide full Federal funding of such part.
H.R.1262 & S.932 - Rep. Michael McCaul (R-TX) and Sen. Markwayne Mullin (R-OK) "Give Kids A Chance Act" - To amend the Federal Food, Drug, and Cosmetic Act with respect to molecularly targeted pediatric cancer investigations. This bill would renew research into pediatric cancers and includes increasing funding for rare diseases, some of which cause Intellual and developmental disabilities and autism.
VOR OPPOSES:
H.R.1 - The One Big Beautiful Bill Act - Rep. Jody Arrington (R-TX) This bill contains provisions to make drastic cuts to Medicaid. The consequences of these cuts could impact HCBS services, further destabilize the DSP workforce, and even impact ICF services. In addition, the bill would add $2.4 billion to the deficit over ten years, which could result in further cuts to safety net programs, including Medicaid, Medicare, and Social Security, in the years to come.
H.R.2743 & S.1332 - Rep. Bobby Scott (D-VA) & Sen. Bernie Sanders (I-VT) Raise the Wage Act - A bill to provide increases to the Federal minimum wage and for other purposes. VOR opposes the provision in this bill that would phase out section 14(c) amd sheltered workshops for indiviiduals with I/DD and autism.
| |
836 South Arlington Heights Road #351
Elk Grove Village, IL 60007
Toll Free: 877-399-4867 Fax: 877-866-8377
| |
FACEBOOK: /VOR ----- TWITTER: @VOR_NET ----- YouTube
| | | | |