|
VOR's Weekly News Update
VOR is a national non-profit organization
run by families of people with I/DD and autism
for families of people with I/DD and autism.
| | |
VOR's Annual Fall Fundraising Campaign!
This is the most important time of year for our fundraising.
Most of our membership renewals and donations
will come in the next eight weeks.
| | |
It's Make-It-Or-Break-It Season for VOR.
Like that little squirrel pictured above, gathering nuts for the months ahead, so it is with VOR.
The contributions we receive in the our fall/winter fundraising campaign cover a significant portion of our expenses in the year ahead.
Please contribute,
so that we may continue to help families like yours.
| | Now Shipping For Thanksgiving | | |
Express your gratitude to the
Direct Support Professionals
in your life
with a little something extra this year...
| | |
Once again, we have partnered with See's Candies in our 2025 Year-End Fundraising Campaign.
See's has agreed to give us a share of the profits for each box sold.
The idea is not to replace our regular appeal for donations,
but to enhance our fundraising efforts by offering delicious See's Candies to our folks who wish to send gifts to family and friends over the holidays.
You may start ordering now.
Candy will begin shipping on November 10, 2025
The last day to order is December 5, 2025
~~ Free Shipping on all orders over $75 ~~
(Except to PO Boxes as extra packaging is required)
| |
Disability Providers Nationwide Considering More Cuts
By Michelle Diament, Disability Scoop, November 10, 2025
With financial pressures mounting, disability service providers across the country are increasingly weighing whether to cut more programs and they say that in-home supports are among their most vulnerable offerings.
A new survey of 469 community-based providers of intellectual and developmental disabilities services in 48 states and Washington, D.C. reveals an industry that is facing added struggles to remain afloat after years of challenges.
Some 52% of providers indicated that they are considering program cuts if recruitment and retention of staff does not improve, according to findings from the annual survey conducted by the American Network of Community Options and Resources, or ANCOR, which represents disability service providers nationally. That’s up significantly from 34% last year.
Service providers have faced growing strain as extra COVID-era funding to support wages for direct service workers expired and federal lawmakers approved a bill over the summer that’s expected to lead to $1 trillion in Medicaid cuts, ANCOR said.
Already, 88% of providers said they experienced moderate or severe staffing shortages in the past year. As a result, 62% said they turned away new referrals and a similar number said they were struggling to achieve quality standards while nearly a third ended programs or service offerings.
In cases where providers cut programs, 42% said they axed residential habilitation services, which enable people with intellectual and developmental disabilities to remain in their homes.
“Even before massive federal Medicaid funding cuts go into effect, our national system of community-based disability services was facing an array of substantial challenges, threatening to undo the progress that had been made in recent years. Add to it the nearly $1 trillion in funding cuts passed earlier this year in the budget bill and it’s not hard to understand why people with disabilities are gravely concerned about the future of their services,” said Barbara Merrill, CEO at ANCOR.
While forthcoming Medicaid cuts do not specify changes to disability services, advocates have warned that people with disabilities will inevitably feel the effects of a dramatic drop in federal investment in the program, especially through optional offerings like home and community-based services.
Continued
| |
The Real Fraud, Waste, And Abuse: Medicare And Medicaid Privatization
By Adam Gaffney, Danny McCormick, Steffie Woolhandler, and David Himmelstein, Health Affairs, November 7, 2025
President Donald Trump and Elon Musk’s Department of Government Efficiency (DOGE) have taken a chainsaw to the US federal government, slashing programs, personnel, research, and global aid. The recently enacted One Big Beautiful Bill Act (OBBBA) budget reconciliation package, meanwhile, cuts nearly $1 trillion from Medicaid and the Affordable Care Act over the next decade—adding more than 10 million to the ranks of the uninsured. The OBBBA also slashes nearly $290 billion from food subsidies for the poor and could trigger $490 billion in cuts from Medicare.
The president and his congressional allies claim these cuts are needed remedies for waste, fraud, and abuse. Yet, they turn a blind eye to the trillions of dollars that private insurers drain from the public Medicare and Medicaid programs. Indeed, one of the administration’s first health financing actions—augmenting payments to Medicare’s private-insurance subcontractors—will add $25 billion to that waste in the coming year alone. If the administration were serious about curbing waste and inefficiency, it would start by reducing the diversion of public funds to these corporate intermediaries.
| |
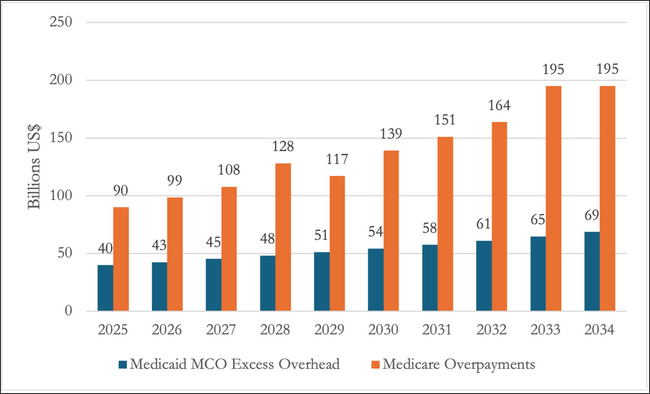
Exhibit 1: Projected savings from eliminating Medicare Advantage overpayments and Medicaid managed care organization excess overhead, 2025–34
Medicaid Managed Care Payments
No official estimates of overpayments to private Medicaid managed care plans are available. However, reliable figures allow calculation of the waste attributable to those plans’ high overhead, which averages 12.54 percent. In contrast, Medicaid overhead across the five states that eschew Medicaid subcontracting is 4.9 percent; the 7.64-percentage-point difference implies that eliminating subcontracting to Medicaid managed care could cut Medicaid expenditures for overhead by $40 billion this year and by $534 billion over 10 years (exhibit 1).
Together, MA overpayments and excess Medicaid managed care overhead will likely cost US taxpayers about $1,920 billion over the next decade. Ending that waste would inflict losses on private insurers’ shareholders and executives (the CEO of the largest MA firm made $26.3 million last year). But patients, not just government coffers, might gain. MedPAC found no evidence that MA coverage leads to better quality care, (a conclusion also applicable to Medicaid managed care according to MedPAC’s sister Medicaid-monitoring commission), while MA plans’ promises of better financial protection and extra coverage have proven mostly empty. Meanwhile, MA’s managed care restrictions limit patients’ care, for example, precluding care at specialized centers (even for patients needing complex surgeries), increasing delays, and apparently increasing mortality.
Waste abounds in US health care. In fact, it far exceeds the $205 billion in savings on waste, fraud, and abuse claimed by DOGE. (That claim is backed by no evidence; most of the savings enumerated on DOGE’s “Wall of Receipts” appear illusory.) Even Congress’ trillion-dollar cuts to Medicaid and food assistance amount to little more than half of the potential savings from de-privatizing Medicaid and Medicare. Reclaiming those funds would require reversing the decades-long trend of outsourcing to profit-seeking intermediaries and restoring Medicare and Medicaid as efficiently administered public programs.
Read the full article here
| |
State Medicaid Officials Project Flat Enrollment Post Unwinding but Increased Spending and Budget Pressures, as States Prepare for Impact of Federal Medicaid Policy Changes
By Chris Lee, KFF, November 13, 2025
As states completed the “unwinding” of pandemic-era continuous coverage, Medicaid enrollment fell 7.6% in FY 2025 and is expected to be largely flat in FY 2026, according to KFF’s 25th annual Medicaid Budget Survey. At the same time, total Medicaid spending grew by 8.6% in FY 2025 and is expected to grow by 7.9% in FY 2026. States report that provider rate increases, greater enrollee health care needs, and increasing costs for long-term care, pharmacy benefits, and behavioral health services are the most significant drivers of increased costs.
In addition to increasing spending demands, slower revenue growth and heightened fiscal uncertainty have created a more tenuous fiscal climate for states in FY 2026. States are also preparing for $911 billion in federal Medicaid spending cuts enacted in the budget reconciliation law earlier this year, including new financing restrictions and work requirements, which will exacerbate existing budget challenges. The challenging fiscal climate and the magnitude of federal Medicaid cuts will make it difficult for states to absorb or offset the reductions.
Almost two-thirds of states say they face at least a “50-50” chance of a Medicaid budget shortfall in FY 2026 as states anticipate state Medicaid spending growth of 8.5% in FY 2026 and tight fiscal conditions. The reconciliation law prohibits all states from establishing new provider taxes or from increasing existing taxes, which could increase state budget pressures. Future requirements to reduce existing provider taxes for states that have adopted the ACA expansion could result in additional budget pressures.
Even though many provisions in the reconciliation law do not take effect until FY 2027 or later, states are already anticipating changes and related fiscal pressures. According to KFF’s companion report, which highlights key policy priorities and issues state Medicaid programs focused on in FY 2025 and are prioritizing in FY 2026, the number of states making reimbursement rate increases for specific provider types is slowing while there is an uptick in rate restrictions. Provider rate changes generally reflect broader economic conditions, and states have typically turned to provider rate restrictions to contain costs.
The survey was conducted in mid-summer of 2025 by KFF and Health Management Associates (HMA) in collaboration with the National Association of Medicaid Directors (NAMD). This year’s estimates of Medicaid spending and enrollment reflect what is assumed in states budgets in most cases, though projections always include some uncertainty.
Read the full article here
| |
Implementation Dates for 2025 Budget Reconciliation Law
From KFF
On July 4, President Trump signed the budget reconciliation bill, previously known as “One Big Beautiful Bill Act,” into law. The bill includes significant health care policy changes. This timeline provides a brief overview of the specific provisions and their effective dates. You can view all health provisions in the order they are implemented or can filter them by the following categories: Medicaid, Medicare, Affordable Care Act and Health Savings Accounts.
[Note: KFF has produced an easy-to-comprehend chart that is too large to print in this newsletter, We recommend our readers view the article on the link below]
Read the full article here
| | |
To better understand the Cuts to Medicaid, CHIP, the ACA, and other Health Provisions, we suggest our readers view this story from The Georgetown University McCourt School of Public Policy
Medicaid, CHIP, and Affordable Care Act Marketplace Cuts and Other Health Provisions in the Budget Reconciliation Law, Explained
By Edwin Park and Sabrina Corlette, Georgetown University McCourt School of Public Policy, August 13, 2025
On July 4, 2025, President Trump signed the Congressional Republican budget reconciliation bill into law (H.R. 1 or P.L. 119-21 which was previously entitled the “One Big Beautiful Bill Act”). Earlier, on July 1, 2025, the Senate passed its version of the budget reconciliation bill on a 51-50 vote (Vice President Vance cast the tiebreaking vote) with the House later passing the Senate bill 218-214 on July 3, 2025. The budget reconciliation law includes numerous provisions related to Medicaid, the Children’s Health Insurance Program (CHIP) and the Affordable Care Act’s Marketplaces, which institute deep, damaging cuts.
According to final Congressional Budget Office (CBO) cost estimates issued on July 21, 2025 the law’s Medicaid and CHIP provisions would cut gross federal Medicaid and CHIP spending by $990 billion over the next ten years. This does not include spending related to a new rural health fund established in the CHIP statute but fully separate from the CHIP program. This also does not account for interactions between provisions of the law and for revenue effects.
Only a handful of these Medicaid and CHIP provisions can be viewed as addressing fraud, waste and abuse but they account for only 2.5 percent of the gross Medicaid and CHIP cuts. States will face significant cost shifts under some of the major Medicaid and CHIP cuts, particularly those restricting state use of provider taxes, at the same time states will face other large cost shifts for SNAP benefits under the law.
Similarly, the law’s provisions related to the Affordable Care Act’s Marketplace eligibility and enrollment policies do nothing to prevent fraud, waste, and abuse. CBO estimates that these provisions would cut gross federal Marketplace spending by an additional $213 billion over the next ten years. This also does not account for interactions and revenue effects.Altogether, the gross Medicaid, CHIP, and Marketplace cuts total $1.2 trillion over ten years. Even accounting for interactions, the net Medicaid, CHIP, and Marketplace cuts equal $1.1 trillion over ten years.
Continued
| |
Opinion: SNAP benefits are a ‘lifeline’ — especially for people with disabilities
By Sara Luterman, The 19th, November 12, 2025
Kajeana Tillman spent the last few weeks not knowing if she would have money to buy her own groceries. She is one of millions of Americans with disabilities who rely on the Supplemental Nutrition Assistance Program, or SNAP.
“I have $3 left on my [SNAP] card right now,” the 51-year-old told The 19th on Friday.
Tillman has a disability but prefers to be identified as “a regular person, just like everybody else.” She lived with her mother until 1996 when her mother passed away. Tillman then lived with her great-grandmother until 2001, when Tillman’s great-grandmother became too old to help care for her.
“I had to get my own place because she needed extra help. So I moved into a residence where I can get help too,” Tillman said.
She now lives in her own apartment in the Bronx. She has a roommate and gets services from YAI, an agency that supports people with intellectual and developmental disabilities. She shops for her own groceries and cooks for herself; Some recent favorites include veggie tots, chicken and salmon prepared in her air fryer.
“I’m trying to eat more healthy food,” she said.The Trump administration’s reluctance to fund the SNAP program during a record-breaking government shutdown has brought intense instability and uncertainty to a program 1 in 8 Americans rely on to be fed. People with disabilities like Tillman disproportionately rely on SNAP to survive.
As the White House has fought in court to block the disbursement of the benefits during the shutdown, some on the right have discussed SNAP recipients by invoking the “welfare queen” stereotype. On Newsmax, anchor Rob Schmitt claimed that women who rely on SNAP “are selling their benefits. People are using them to get their nails done, to get their weaves and their hair.” AI-generated videos of angry Black women have proliferated on social media platforms like TikTok. Rep. Clay Higgins, a Republican from Louisiana, suggested that people harmed by SNAP disruptions should “stop smoking crack.”
“It’s a deliberate demonization of something that is a lifeline for people,” said Hayley Brown, a labor and disability researcher at the left-leaning Center for Economic and Policy Research.
Tillman needs significant support to live her life, and people with disabilities like her have been largely absent from the public conversation.
She and other YAI clients have staff who check in on them throughout the week and who can support them in tasks like money management, grocery shopping and medical appointment follow-ups. YAI supports 590 people with intellectual and developmental disabilities like Tillman in living in their own apartments. Eighty-five percent of them, including Tillman, rely on SNAP.
It is difficult to know precisely how many disabled adults nationwide rely on SNAP because of how the data is collected and recorded.
“Food insecurity is defined by the federal government at the household level rather than at the individual level. That could be a single person household with a disability. It could be a parent with a child with a disability, somebody else living in the household with a disability,” said Craig Gundersen, a professor of economics at Baylor University.
Those living in a household with at least one disabled person experience rates of food insecurity about double those without. A recent analysis released by the Center for Economic and Policy Research and authored by Brown showed that 20.4 percent of households containing at least one person with a disability rely on SNAP, versus 8.3 percent of those without.
This is, according to Brown, “a very conservative estimate.”
Continued
| |
Opinion: Recent Actions by the Trump Administration Target Children with Disabilities
By Lily Klam, First Focus on Children, November 12, 2025
Proposed rules, reductions in force, threaten roughly 100,000 children who rely on Supplemental Security Income, plus others in need of support and services at school, at home, in health care.
Supplemental Security Income, or SSI, is a lifeline for children with disabilities whose families have limited income and resources. Kids who rely on this benefit are now in the crosshairs of a new proposed rule from the Social Security Administration that estimates suggest could make it more difficult for as many as 100,000 children to qualify and stay qualified for their full monthly SSI benefit.
The proposed changes to SSI appear to be part of a larger agenda by the Trump Administration to disenfranchise children with disabilities. For instance, during the recent government shutdown, the Office of Management and Budget carried out massive reductions in force (RIFs) at agencies that oversee the majority of programs for children, and specifically targeted the Department of Education (ED) and the Department of Health and Human Services (HHS), which serve large proportions of children with disabilities.
In addition to supporting basic needs such as food and housing, SSI helps cover the extra costs of raising a child with a disability, such as medical care, therapies, adaptive equipment, and transportation. For many families, SSI means the difference between stability and poverty, and allows children to grow up at home, stay connected to their communities, and access the care they need to reach their full potential. Nearly 1 million kids with disabilities — ranging from mental and neurodevelopmental conditions, musculoskeletal disorders such as cerebral palsy and muscular dystrophy, nervous system disorders such as epilepsy, and vision or hearing impairments — rely on SSI to meet their basic needs.
The rules to qualify and stay qualified for SSI are complex, both for the beneficiary to follow and for the Social Security Administration to administer. One of the most complex rules concerns “in-kind support and maintenance” or “ISM.” This rule reduces a beneficiary’s monthly SSI benefit by as much as one-third if they receive support from a family member or loved one, including groceries or a place to stay.
Under current rules, children are exempt from this reduction to their SSI benefit when anyone in their household qualifies for certain public assistance programs, including SNAP. This exemption makes the program easier for SSA to administer and it means that SSI beneficiaries have less burdensome red tape to worry about. It also allows generational families to stay together and to administer care for elderly or disabled relatives under one roof without jeopardizing the benefits they need to make ends meet, or having to move anyone — either their child or disabled relatives — into institutionalized care.
Proposed rule signifies a major shift in policy
The Trump Administration’s proposed rule would eliminate SNAP from the list of programs that qualify households for the ISM exemption. It also would require all members of the household to qualify for public assistance, not just one member. This change would subject as many as 400,000 SSI beneficiaries — a quarter of them children — to benefit reductions or, in many cases, the complete loss of benefits altogether.
The proposed rule is more than just a technical change in regulatory definition: it signifies an enormous shift in policy that will have serious implications for kids with disabilities. It will mean less stability and less of a financial cushion for caregivers to provide food and clothing, let alone therapies, adaptive equipment, home modifications, and other supports that these kids need to survive.
SSI’s statutory eligibility rules have gone without updating for more than 40 years, and lawmakers have finally secured bipartisan support to move the program forward for the first time in decades. This change in regulatory policy represents a huge step backward.
Children with disabilities bear the brunt of Trump Administration policy
The Trump Administration has not been favorable to children in general. President Trump has promoted and signed into law massive cuts to children’s health care, food assistance and other critical programs. During the recent government shutdown, low-income children were singled out when the Administration went all the way to the Supreme Court fighting to withhold SNAP funding they’d been compelled to release.
Children with disabilities appear to be taking the brunt of many Trump Administration actions. In addition to the proposed changes to SSI benefit regulations, the Trump Administration gutted the Office of Special Education and Rehabilitative Services (OSERS) during last month’s RIFs, leaving it with just a handful of staff. OSERS is responsible for monitoring compliance and distributing funding for the Individuals with Disabilities Education Act (IDEA), the key law protecting the rights of students with disabilities in schools. These layoffs jeopardize the ability of ED to administer IDEA funding and to enforce protections for students with disabilities in schools.
Continued
| |
Federal special education staff may get their jobs back. But for how long?
By Cory Turner, NPR, November 13, 2025
The deal Congress reached to re-open the federal government requires the Trump administration to reinstate federal workers who were fired in October, including those charged with overseeing the nation's special education laws. But it's not clear how long they'll be back.
As NPR has reported, the Office for Special Education and Rehabilitative Services (OSERS) inside the U.S. Department of Education is the central nervous system for programs that support students with disabilities. It not only offers guidance to families but also oversees state compliance with the Individuals with Disabilities Education Act (IDEA).
OSERS can't do its job without staff, and, according to a new Education Department filing, the office lost 121 of its 135 employees in the October reduction-in-force. That matters because, while Wednesday's funding agreement will return those workers to "employment status" as of Sept. 30, there appears to be little protecting them after Jan. 30, when that provision expires.
"We are concerned special education will cease to exist," says Jacqueline Rodriguez, CEO of the National Center for Learning Disabilities.
The Education Department did not answer specific questions from NPR about whether workers who were cut in October would be allowed to resume their work, as opposed to being put on administrative leave, or if the department would try to fire them again after the deal expires.
The Office for Civil Rights has also seen big cuts
Another Education Department office that supports students with disabilities was also decimated by the October cuts.
Families often turn to the Office for Civil Rights (OCR) when they fear their child has been illegally denied special education services. But the Education Department's recent court filing shows the extent of the administration's efforts to gut that office:
OCR lost 299 staffers after the March reduction-in-force but, because of a lawsuit, most (247) remain on temporary, paid administrative leave. Another 137 were cut in the October reduction-in-force, which has been paused by a federal judge. Under the new government funding agreement, those 137 staffers should be reinstated, at least until Jan. 30.
By the department's own numbers, that means just 62 staffers of OCR's current 446 employees have not received RIF notices. That's roughly 10% of the office's 600-plus headcount in January, when the second Trump administration began.
OCR and OSERS are both mandated by federal law.
Read the full article here
| |
30 Years Without A Real Raise: Early Intervention Pay Crisis
By Sarah Carr, The 74 via Disability Scoop, November 13, 2025
When, in the 1990s, Emily Lengen chose a career working with babies and toddlers with disabilities, it felt like a chance to earn decent money while doing important, challenging work that she loved. Lengen, who lives near Rochester, N.Y., travels in person to the families’ homes — sometimes logging up to nine visits in a day — teaching children with developmental delays and disabilities how to play with toys and socialize with siblings and peers; and coaching their parents in how to help the babies grow and thrive.
Yet as her 30th anniversary working as a special education teacher for the New York State Early Intervention Program approaches, Lengen increasingly feels disillusioned: still happy in her work, but distraught about remaining in what may be the only profession in New York that hasn’t gotten a substantive raise — in absolute terms, much less adjusting for inflation — in three decades. Any modest rate increases the state’s early intervention providers (which include teachers like Lengen and a range of therapists) have benefited from, were generally counterbalanced by cuts. “As a 30-year veteran with a master’s degree, I am working twice as hard as when I started in early intervention, and making less now,” Lengen said.
Over the same time period, New York’s hourly minimum wage has more than tripled, from $4.25 in the mid-’90s to more than $15 now. The average salary for public school teachers jumped from about $48,000 in the mid 1990s to about $95,000 in 2023-24, according to the National Education Association. And, while New York state data is elusive, nationally the average compensation package for chief executives climbed from nearly $6.4 million in 1995 to more than $20 million in recent years.
The Economic Policy Institute’s Elise Gould, who researches wages and economic inequality, said she knows of no precedent for a job where the absolute pay hasn’t risen in 30 years. “It’s a little hard to believe,” she said.
Early intervention providers deliver critical services including speech, physical and occupational therapy to children from birth through age 3 who have a range of developmental delays and disabilities. When done well and promptly, research shows that it can reduce the need for costly special education services, as well as other public assistance down the road, and improve life outcomes.
Early intervention systems are state-led and designed, and the mix of specific funding sources can vary considerably across states. New York relies on a combination of private insurance dollars and county, state and federal funding, including Medicaid, to serve approximately 70,000 children.
Many of the therapists, special education teachers and others who provide early intervention services are not salaried employees. In New York, they are paid a fee for service rate that is set by the state. After providing the service, they submit a claim for reimbursement and are paid either by Medicaid if the child is eligible, or by the state, which draws from a combination of funding streams.
For many services, including the specialized therapy and support that Lengen provides, that rate was higher in the 1990s when early intervention began in New York state, than it is today.
Continued
| | |
The following articles are a three-part series on abuse and neglect in New Hampshire's system for people with intellectual and developmental disabilities. Click here to access the full series.
A series of tragedies exposes patterns of abuse and neglect in New Hampshire’s disability system
By William Skipworth, New Hampshire Bulletin, November 10, 2025
| |
A VIDEO RECORDED at a Dunbarton care home for people with intellectual and developmental disabilities in February 2019 captured caretakers pinning Lucas Houle to the ground and slapping him repeatedly. Amid his pain and fear, Houle made a tearful plea: “I want to go home.”
Four months later, Christine Marie Bill was found dead after several hours in a hot, sealed car in Andover, according to the lawsuit filed in the wake of her death and a State Police incident report. Bill, due to her cognitive disabilities, had a history of leaving the house, and it was her caretaker’s job to check on her every 15 to 30 minutes.
In March 2023, a woman named Laurie Raymond, who has cerebral palsy and is nonverbal, was living at a residential facility in Lyme when she suffered second-degree burns to her abdomen, legs, and genital area. A registered nurse caring for Raymond placed her under scalding water and then scrubbed the burns, resulting in a $45,000 medical bill, according to a malpractice lawsuit filed by the family.
While every story of abuse and neglect within New Hampshire’s intellectual and developmental disability care network is unique in the harm caused, collectively they point to the state’s systemic failures in oversight and accountability. Over the past several months, the Bulletin has learned about people like Houle, Bill, Raymond, and others through court filings, law enforcement documents, state records, and conversations with lawyers, advocates, and family members. Their stories are being reported for the first time here. Each individual tragedy is illustrative of the consequences of repeated breakdowns in care — care that is paid for and overseen by the state.
According to state records obtained by the Bulletin, New Hampshire investigated 1,405 complaints of abuse, neglect, and exploitation committed against people with intellectual and developmental disabilities receiving state services from January 2023 through the first six months of 2025. Of those, 467 were deemed credible after a state investigation, according to the records. Some of those complaints include physical and sexual abuse. Eighteen of the complaints were withdrawn before the investigations were complete, and 28 complaints were ongoing investigations when the records were produced.
Additionally, state records show 119 people died in New Hampshire’s intellectual and developmental disability system from January 2023 through the first six months of 2025. Of those deaths, 79 were deemed “anticipated” by the state — state officials wouldn’t answer the Bulletin’s questions about how they defined anticipated — and at least 22 were categorized under “unknown” cause of death.
Holly Haines, a Manchester attorney who represented the Bill family, said that case taught her a lot about New Hampshire’s disability care system.
“The state is hiring vendor private agencies,” she said. “The private agencies are hiring private people, and not training them or educating them adequately, and it’s ultimately the disabled individuals who are harmed.”
There is more “fingerpointing,” she said, than taking responsibility.
“I don’t think the state knows what’s actually going on in the households,” Haines said. “I’m not sure the vendor agencies even are aware.”
In a written statement issued in response to the Bulletin’s requests for an interview with Department of Health and Human Services Commissioner Lori Weaver, among other state officials, for this investigation, DHHS spokesman Jake Leon said that the department can’t comment on individual cases but “has a process in place to review and investigate complaints made against providers and vendors licensed or certified through the Department.”
The office of Gov. Kelly Ayotte shared a similar statement: “DHHS has a process in place to review and investigate complaints, and the Governor will be monitoring this issue closely.”
Continued
| |
A man with disabilities was found dead in the woods. New Hampshire was supposed to protect him.
By William Skipworth, New Hampshire Bulletin, November 12, 2025
THEY CALL IT the disability cliff.
When young people with intellectual and developmental disabilities finish high school, they lose access to the extensive services provided by public school special education programs. Most parents work, and while that allows them to help support their adult children financially, their absence creates a care void that is not easy to fill.
Over many months, the Bulletin has explored abuse and neglect in New Hampshire’s intellectual and developmental disability system through court filings, law enforcement documents, state records, and conversations with lawyers, advocates, and family members. Breakdowns in care in recent years have led to many instances of preventable harm — sometimes fatal harm — and left in their wake devastated families who wanted only to give their children opportunities for a good life but found tragedy instead.
Those tragedies often begin at the precarious edge of the disability cliff — and that was the case for the Weidlich family.
When Stephen “Stevie” Weidlich Jr. aged out of high school in 2017 at Crotched Mountain School for Students with Disabilities in Greenfield, his father, Stephen Weidlich Sr., saw few options.
Weidlich worked full time and Stevie’s mother wasn’t involved in his life. He considered trying to get designated by the state as an in-home care provider of state services, which would have allowed him to receive some Medicaid funding as Stevie’s caregiver. Such arrangements typically cost the government a fraction of what placement in a residential facility costs.
However, the family felt discouraged about pursuing that path when an employee of PathWays of the River Valley, one of 10 agencies designated by the state Department of Health and Human Services’ Bureau of Developmental Services to coordinate care for people with disabilities, stopped responding to their inquiries on the matter, Weidlich said in a recent interview.
The one option that remained was to place Stevie in a home run by PathWays with a live-in caregiver, a service people with intellectual and developmental disabilities are legally entitled to receive through Medicaid and other state and federal dollars.
Within a few years, Stevie would become a casualty of that system. In December 2022, police knocked on the Weidlich family’s door in Unity to tell them Stevie’s body had been found in the woods behind the home of his caregiver.
At the time of his death, Stevie, 26, was living in Allenstown with PathWays employee Douglas Onkundi.
As a live-in caregiver, it was Onkundi’s responsibility to ensure Stevie, who had physical, developmental, and intellectual disabilities, was given 24/7 care. However, according to documents from a state investigation obtained and being made public for the first time by the Bulletin, Onkundi wasn’t actually living in the home at the time of Stevie’s death. He told police he was living in Manchester, and would return to Allenstown to give Stevie his medications. In his stead, investigators learned, Onkundi was paying another man to live in the home and care for Stevie with part of his PathWays paycheck and pocketing the rest. The man had no formal training and was not officially authorized by Pathways or Stevie’s family. Neither Onkundi nor the other man were criminally charged.
In conversations with state investigators, PathWays managers said they’d told Onkundi on multiple occasions only trained staff can work with the people in their care. However, according to the report, Onkundi said there was “an unwritten rule that everything was OK unless PathWays said otherwise.”
On Dec. 18, 2022, security camera footage from a neighbor shows Onkundi leaving the home in the morning and returning around 8 p.m. the day Stevie died, per the report.
Investigators were told Stevie had locked himself in the bedroom and that when Onkundi returned, he used a ladder to climb up to the window and discovered the glass was broken and Stevie was gone. Onkundi told state investigators he searched for Stevie, who had a history of fleeing, before calling police.
It was too late. A police dog found Stevie’s body in the woods behind the home. There was evidence of hypothermia and a blunt force injury to Stevie’s ribs consistent with either a fall or a blow to the chest, the police report said. It was a cold night with snow on the ground.
~~~~~~~~~~~~~~~
The Incapacitated and Vulnerable Adult Fatality Review Committee is a board of experts established through state law to review concerning deaths of vulnerable or incapacitated people, evaluating if there were any failures in state policy or practices that led to the death. The board then makes recommendations on how to prevent future similar deaths.
Both co-chairs of that committee, Vanessa Blais and Francesca Broderick, told the Bulletin Stevie’s death was never brought before the committee. Agencies like the Bureau of Aging and Adult Services and Department of Health and Human Services — which both knew of the death and have representatives on the committee — aren’t legally obligated to report deaths to the committee. They’re merely encouraged. Still, when the Bulletin told her about Stevie’s death, Blais said she was shocked it hadn’t been brought to her committee.
Attorneys Kristin Ross and Cristina Rousseau, who are representing Weidlich in his lawsuit and have represented multiple families in this system, said tragedies like Stevie’s are symptomatic of a broken system.
“Really what we see is a lack of accountability and a lack of consequences when things go wrong within the area agency system, and frankly I think that starts at the top,” Ross said. “There are regulations that are supposed to be being followed, but what we find is they’re not, and there’s no consequences, and there’s a very laissez-faire attitude about the fact that they’re not being followed.”
In Stevie’s case, Rousseau noted the entire investigation focused on Onkundi.
“But you know what has never happened in any of the cases we’ve been involved (with)?” Rousseau said. “The area agencies are not investigated. They are the ones that have all of these duties, and when it comes to violations that have occurred, nobody looks at PathWays.”
Rousseau and Ross also point to what they consider a perverse financial incentive within the system of care.
“Something that we’ve seen is a pushback against allowing immediate family members to become the approved in-home care providers,” Ross said. “And instead a push towards individuals outside of the family.”
Agencies and caregivers earn significantly more money providing residential care than day services. According to PathWays’ contract with Onkundi, acquired by the Bulletin, Onkundi was paid more than $5,000 per month and more than $62,000 annually to care for Stevie. Had he been providing day services, he would’ve been paid about $1,400 a month and $17,000 annually, according to the contract.
Read the full article here
| |
New Hampshire’s disability system has a horrific past, and advocates say the path forward is unclear
By William Skipworth, New Hampshire Bulletin, November 14, 2025
IN 1956, A DOCUMENTARY titled “Help Wanted” placed viewers inside the Laconia State School, which from its founding in 1903 as the New Hampshire School for Feeble-Minded Children to its closure in 1991 housed people with disabilities.
So disturbing were the visuals that the Portsmouth Herald compared the institution to images of the concentration camps of Nazi Germany.
Overcrowding plagued the New Hampshire facility, with over 1,000 residents by 1942, according to a historical account from the Laconia Daily Sun. There was no privacy or personal space in the group bedrooms — and in one building a single toilet was shared among 80 people. Many residents were forcibly sterilized, and beatings were routinely given as punishment for bad behavior.
For nearly a century, the institution served as the state’s response to the needs of people with disabilities. It took a class-action lawsuit — and its articulated horrors — to shutter the place for good and usher in a new system for state-administered care more than three decades ago.
But as a monthslong Bulletin investigation into New Hampshire’s modern disability care network has revealed, systemic problems of abuse and neglect haven’t gone away. Tragic story after tragic story — many of them reported this week for the first time — provide the evidence.
~~~~~~~~~~~~~~~~
In New Hampshire, people with intellectual and developmental disabilities are entitled to services. The state designates 10 area agencies, including the Moore Center, to either provide this care or subcontract with another vendor agency, such as Community Integrated Services, to do so. The area agency system, established in the wake of the Laconia State School, is overseen by the state’s Department of Health and Human Services’ Bureau of Developmental Services and is paid for by Medicaid and other state and federal dollars.
Gov. Kelly Ayotte told the Bulletin on Wednesday that after the first two parts of this series were published, she reached out to DHHS Commissioner Lori Weaver and Attorney General John Formella to discuss the issues raised.
“These are very serious allegations,” Ayotte said. “They need to be examined, and we need to make sure that the system is serving the people that have disabilities in our communities, and also any of the contractors, the area agencies that contract with the state to serve people with disabilities, make sure that they are performing and that they are treating people well, so I take this very seriously.”
She said she will “continue to make sure that these are investigated, that we follow through with any changes that need to be made to the system.”
~~~~~~~~~~~~~~~~
Rampant abuse and neglect
State records obtained by the Bulletin show New Hampshire investigated 1,405 reports of abuse, neglect, and exploitation committed against people with disabilities in the state’s intellectual and developmental disability system from January 2023 through the first six months of 2025.
Those reports include allegations of physical attacks, sexual abuse and assault, and verbal attacks committed by staff against people with disabilities in their care. Of the reports, 467 were deemed credible after a state investigation, according to the records, while 18 of the complaints were withdrawn before the investigations were complete and 28 complaints were ongoing when the records were produced.
State records also show 119 people died in New Hampshire’s disability system from 2023 through June 2025. Of those deaths, 79 were deemed “anticipated” by the state (state officials refused to define “anticipated” for the purposes of these records) and at least 22 were categorized under “unknown” cause of death. The causes of death in the records include “intracranial hemorrhage” (brain bleed), complications from a “right femur fracture,” and “probable bacterial infection, and malnutrition.”
No further information is included in the records that would provide more context, and the state declined to provide the Bulletin with further documentation on the deaths even with personally identifying information redacted, citing state statutes.
News reports from other states — including Missouri, West Virginia, and California — suggest New Hampshire is not entirely unique, as abuse and neglect have been reported elsewhere. Additionally, the Bulletin collected data from neighboring states on their developmental disability systems through a series of open records requests. However, differences in how data is categorized and reported — as well as population variations — make comparisons with bordering states challenging.
In Vermont, 92 people died within the state’s intellectual and developmental disability system in 2023 and 2024, according to state records. In Massachusetts’ system, 730 people died in 2023 and 2024.
Massachusetts categorized the deaths even further: 18 were determined to be accidental, one cause was undetermined, and 21 were still pending investigation earlier this year when the records were produced. The remaining were attributed to natural causes. In Maine’s system, 112 people died in 2023 and 2024, per state records. Of those deaths, three were accidental and 56 were attributed to “unknown causes.”
As for abuse and neglect, Vermont saw 680 instances of “alleged abuse, neglect, and prohibitive practices” and 254 “criminal acts” in 2023 and 2024, per state records. In Massachusetts, records show 11,652 complaints of abuse and neglect in 2023 and 2024. And in Maine, there were 370 complaints of abuse and neglect in 2023 and 2024.
Read the full article here
Click here to access the full series.
| |
In NJ, managed care means delays and denials for disabled patients: 'Not a fair fight'
By Gene Myers and Scott Fallon, The Bergen Record (NorthJersey. com) November 6, 2025
Josh Gargano knew what would happen when his therapy was cut.
His body would seize up. Without regular physical and occupational therapy, his spastic quadriplegia — a severe form of cerebral palsy — would lead to increased stiffness, reduced mobility and, eventually, chronic pain.
“You take these services away, I regress,” said Gargano, 35, who uses a wheelchair. “You put me back on them, I improve. It’s as simple as that.”
Like many New Jerseyans with disabilities, Gargano's care is funded by the state's Medicaid program. But in April of 2023, United Healthcare, the private managed-care company that administers his coverage, announced that it would be cutting his in-home nursing care from 16 hours a week to eight.
The two sides eventually compromised, but it followed a months-long fight in which the insurer overruled Gargano’s own doctor and nurse. In the interim, Gargano lost control of his neck muscles and developed an abscess due to his immobility, his mother said.
Gargano's plight highlights problems that many with disabilities complain about under New Jersey’s Medicaid managed-care system, in which five private companies oversee the publicly funded, $22.5 billion-a-year program.
In our Hurdles to Health Care series, The Record and NorthJersey. com have examined the many challenges disabled patients face in getting good care, from inaccessible clinics to poorly trained doctors and inadequate insurance payments.
The Medicaid managed-care system may be among the most pervasive obstacles. The system gives insurers wide latitude to decide who gets essential services like therapy and in-home nursing. Families say the result is often denials and delays — and opaque reasoning.
How Medicaid managed care works
Disability advocates say Medicaid managed-care organizations, known as MCOs, lean on proprietary assessment tools, force families through multilayered appeals and still prevail even when doctors deem treatment “medically necessary.”
“This system has tilted too far in favor of the insurance companies,” said Paul Aronsohn, New Jersey’s ombudsman for people with intellectual and developmental disabilities. “It’s too easy for them to say no, and too hard for families to push back.”
The state contracts with five MCOs: United Healthcare, Horizon Blue Cross Blue Shield, Aetna, WellCare and Wellpoint (formerly Amerigroup). Together, they administer NJ FamilyCare, New Jersey's Medicaid program, which covers 1.8 million low-income and disabled residents.
In the U.S., where per-person health care spending is far higher than in the rest of the world, managed care has been touted as a way to control costs. New Jersey gives insurers a fixed monthly payment for each enrollee. Companies are expected to manage an individual’s care within that budget. The goal is to control costs and improve coordination.
Horizon Blue Cross Blue Shield, the MCO with the most enrollees, says it follows state guidelines for denials and appeals and participates in regular quality reviews. By law, a spokesman noted, MCOs must spend at least 85% of premiums they collect on medical care.
Critics in the disability community argue that the industry too often treats that 85% as a ceiling for medical spending, not the floor it should be. Profit incentives and weak oversight by the state skew decisions toward cutting care, they say.
Patients and their loved ones often feel that the appeals process is stacked against them. While managed-care insurers, by law, must provide a formal process to challenge denials, families often find themselves battling insurance company lawyers on their own, even as they continue to care for children with complex medical needs.
“Even when families win an appeal, the decisions aren’t binding,” noted Aronsohn, the disability ombudsman. “It’s not a fair fight.”
Since his appointment in 2018, his office has tallied numerous complaints from families like the Garganos and Wrights who say their Medicaid-funded care, such as private duty nursing or personal care assistants, was cut or denied without clear justification. MCOs use assessment tools that aren’t publicly available, even to his office, Aronsohn said.
“Families have no idea what criteria are being used,” he added.
Read the full article here
| |
Ohio Senate passes bill assisting adults with developmental disabilities
SB 35 recognizes 'supported decision-making as an alternative to guardianship'
By GQLSHARE, The Morning Journal, November 13, 2025
Following recent unanimous approval in the Senate Judiciary Committee, the Ohio Senate also passed Senate Bill 35 unanimously, which recognizes “supported decision-making” as an alternative to guardianship for adults with a developmental disability.
Supported decision-making is the process of helping and accommodating an adult with a developmental disability who is making, communicating, or carrying out their own life decisions without impeding their self-determination.
A written supported decision-making plan must be signed and voluntarily acknowledged by the principal, without coercion or undue influence.
Additionally, the measure states that individuals are “presumed capable of making decisions about their lives and activities of daily living and are competent to handle their own affairs,” unless a court determines otherwise.
“All of us look to family members and friends for help with decisions at different points in our lives, and this bill allows adults with developmental disabilities to do the same,” said Sen. Jerry Cirino, R-Kirtland, who jointly sponsored the legislation with Sen. Michele Reynolds, R-Canal Winchester.
“Supported decision-making protects adults with developmental disabilities from exploitation because they are able to maintain control over their own lives,” he added. “The provisions included in this bill help to maximize the state’s guardianship resources for those who truly need them.”
Moreover, the bill requires the Ohio Department of Developmental Disabilities to create a standard written supported decision-making plan that can be used by a principal and one or more supporters.
Continued
| |
'We’re scared': Texas providers urge state to reconsider Medicaid cuts to medical supply services
By Abigail Ruhman, KERA News (NPR), November 10, 2025
Providers warn proposed cuts to Texas' Medicaid reimbursement rates could hurt medical supply companies and the patients that rely on them.
The Texas Health and Human Services Commission is proposing significant cuts to reimbursement rates for dozens of services provided through Medicaid, like ventilators and wheelchairs. Providers said during a public hearing Monday the cuts could reduce access to services or lead to closures.
Stephen Hernandez, director of operations at Angel Medical Supply in Houston, said these cuts could lead to a decrease in vital support for patients throughout Texas.
“Everybody in here is scared,” Hernandez said. “And if we're scared, imagine how the patients feel.”
Hernandez was one of dozens of providers who asked HHSC to reconsider the new rate proposals for services related to feeding tubes, mobility aids and respiratory care. Angel Medical Supply serves patients within a 100-mile radius of Houston. Hernandez said these cuts could lead to companies like his limiting what services they provide and who they can provide the services to.
The proposed changes would reduce reimbursement rates for some services by more than half, with some cuts reaching up to 85%. If approved, majority of the cuts would go into effect next year.
Stephen Vigorito’s son uses a feeding tube known as enteral nutrition. That service would face a cut of more than 44%.
“There are no other alternatives except for him to go on a continuous feed... instead of the feeding pump, which means a decreased quality of life,” Vigorito said. “It appears that there's like this calculus, like how can we reduce [medical supply company] profit enough to where they'll still stay in business but just limp along.”
Medical supply companies, also known as durable medical equipment or DME businesses connect people to devices they may need – and provide support if people have an issue with the device. For example, if a ventilator were to malfunction, they often act as service technicians.
While patients can purchase certain equipment from larger companies, many don’t offer the level of support life-sustaining devices can require.
Many providers in Monday’s hearing noted lower reimbursement rates could mean these local companies would also have to limit the maintenance services they offer.
Thomas Suniga, A&P’s director of quality control and product analysis, said these cuts could end up costing the state more in the long run by increasing the administrative burden on providers and leading to more hospitalizations.
“I get those calls at 4 o'clock in the morning from a hospital asking what's going on. We have to step in and act,” Suniga said. “We don't have time to wait around for paperwork and things like that. We have to jump in and treat patients right away.”
Suniga also said increased hospitalizations could lead to longer waiting times for everyone.
Read the full article here
| | |
VOR's Irene Tanzman (and Founder of the Saving Wrentham and Hogan Association) appears on the Kevin, M.D. Podcast
A question about maternal health and the rise in autism [PODCAST]
KevinMD Podcast, November 13, 2025
Patient advocate and author Irene Tanzman discusses her article “A mother’s question about PCOS and her son’s autism.” Irene shares her personal journey as a mother to a son with severe autism and intellectual and developmental disabilities (IDD), exploring the challenging but necessary questions about the link between maternal PCOS (polycystic ovary syndrome), the modern metabolic crisis, and fetal neurodevelopment. Irene advocates for looking “upstream” at maternal health before conception, questioning if fertility treatments are addressing the underlying hormonal environment needed for optimal development. This episode dives into the realities of caregiving for severe autism, the need for better pre-conception support for women with PCOS, and the urgent call for a broader, more honest public health conversation. Learn why exploring maternal metabolic health is a critical, compassionate step toward understanding autism.
Listen to the Podcast here
| |
Acute effects of cannabis on core and co-occurring features associated with autism spectrum disorder in adults
By Debra Kahrson, Emily M. LaFrance, and Carrie Cuttler, Nature - Scientific Reports, November 13, 2025
Abstract
Pharmacological interventions that treat core and co-occurring features of autism spectrum disorder (ASD) are a persistent unmet need. As such, use of cannabis to manage ASD features is common in the autistic community. Yet, few studies have examined the acute effects of cannabis on symptoms associated with ASD. Therefore, we measured changes in symptom ratings from before to after cannabis use in a sample of 111 self-identified autistic adults. Anonymized archival data sourced from the Strainprint® app were analyzed. A subset of tracked information that reflected changes in core and co-occurring symptoms associated with ASD (i.e., Sensory Sensitivity, Repetitive Behaviors, Mental Control, and Negative Affect) were used to assess the impacts of cannabis on symptom severity. Overall, symptom severity ratings were reduced by 73.09% from before to after cannabis use. More severe symptoms were associated with greater reductions in severity ratings after use. Higher doses predicted greater reductions in severity of Repetitive Behaviors, Mental Control, and Negative Affect but dose of cannabis used to manage all symptoms remained static across time. Results from this first empirical examination of the perceived acute effects of cannabis in autistic adults suggest that cannabis provides temporary relief from symptoms associated with ASD.
Results
Cannabis use characteristics
Table 2 displays cannabis use characteristics for the entire sample, and for each symptom cluster. Specifically, the table displays descriptive statistics pertaining to dose of cannabis used (# of puffs), as well as THC and CBD concentrations (measured in %) in the cannabis used to manage each symptom cluster. A small number (n = 88, 1.48% of total sessions) of lab-verified tracked sessions measured THC and CBD concentrations in mg/dose, mg/inhalation, or mg/ml, or did not list the measurement scale. These sessions were excluded from analysis of mean THC/CBD content listed in Table 2, as well as latent change score analyses where the influence of dose, %THC, and %CBD were included as predictors of change in ASD symptom severity.
| |
Overall change in symptom severity ratings
ASD symptoms were reported as being reduced (as opposed to exacerbated or unchanged) in the vast majority of tracked sessions (98.33%). With respect to each symptom cluster, Sensitivity symptom ratings were reduced in 97.26% of tracked sessions, ratings of Repetitive Behaviors were reduced in 99.71% of tracked sessions, Mental Control symptom ratings were reduced in 97.68% of sessions, and Negative Affect symptom ratings were reduced in 98.40% of sessions.
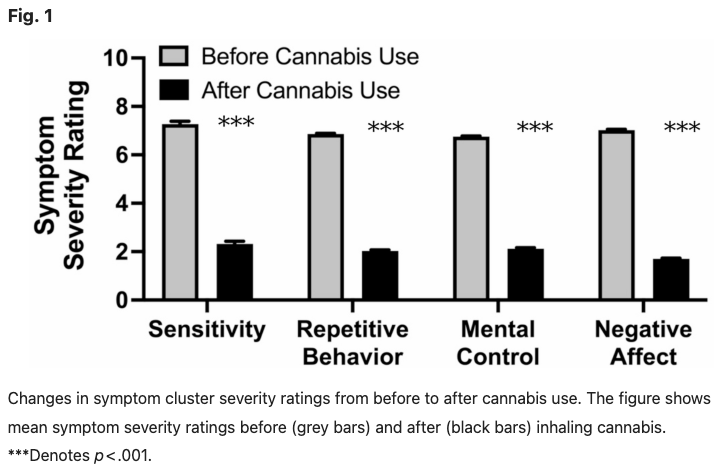
As further depicted in Fig. 1, mean Sensitivity severity ratings were significantly reduced from 7.27 (SE = 0.12) to 2.32 (SE = 0.11) (p < .001) which represents a decrease of 68.09% from before to after cannabis use. Similarly, ratings of Repetitive Behavior severity were significantly reduced from 6.86 (SE = 0.03) to 2.03 (SE = 0.04) from before to after use (p < .001) (representing a 70.41% reduction). Ratings of the severity of problems with Mental Control were significantly reduced from 6.75 (SE = 0.03) to 2.12 (SE = 0.04) (p < .001) which indicates a 68.59% reduction, and ratings of the severity of symptoms of Negative Affect were significantly reduced from 7.02 (SE = 0.03) before cannabis use to 1.70 (SE = 0.03) after cannabis use (p < .001) representing a 75.78% reduction in severity of this symptom cluster. Collapsed across all three symptom domains, symptom severity ratings were reduced from a mean of 6.95 (SE = 0.02) before cannabis use to 1.87 (SE = 0.02) after cannabis use which represents an overall reduction in all symptom ratings combined of 73.09%.
Read the full report here
| | |
The final two articles in this week's newsletter illustrate the media's never-ending resurrection of America's history of warehousing of people with I/DD and autism with implications that any form of institutional care is a continuation of this abusive system.
While we obviously disagree, we find it important to share these articles to let our readers know that they continue to be printed, and that this is what VOR must continue to confront.
| |
UConn grapples with the legacy of a CT institution for the disabled
By Emily Otte, CT Mirror, November 9, 2025
For decades, the Mansfield Training School site has been vacant. Now, a small group of researchers seeks to memorialize it.
English professor Brenda Brueggemann had driven by the memorial stone, the grassy grove and the architectural shells of the shuttered institution every day for years on her way to teach at the University of Connecticut.
The campus of the former Mansfield Training School, a state institution that, until the early 1990s, had housed people with intellectual disabilities, was now nothing more than a labyrinth of empty buildings along a stretch of Route 44, overgrown with ivy and left to rot on the inside.
Then in 2022, a student of Brueggemann’s, who was researching how individuals with disabilities were treated in university settings, started digging through UConn’s archives. The work would lead to what Brueggemann called a “dark realization” about the history that was hiding in plain sight.
And it launched a much larger project.
For the past three years, Brueggemann and her students have been piecing together the history of the Mansfield Training School, now owned by the university and referred to as the “Depot Campus.” They’ve gone through archives, given presentations, made visits to the site and created a website outlining the history of the training school and what they’ve found in its archives. And they’ve grappled with its controversial legacy — one that aligns with the fraught history of institutions for disabled people across the U.S.
Brueggemann has also taken on the task of piecing together an oral history of the Mansfield Training School. She’s spoken with family members of former residents and, through a Facebook group, she’s interviewed people who used to work there. Now she’s looking for a way to formally preserve it all.
“The more I found, the more I knew that we needed a memorial of some kind,” Brueggemann said.
The student who first called Brueggemann’s attention to the vacant campus was Jess Gallagher. Then an undergraduate student in English literature, Gallagher was working on an honors thesis and had been reading about the way people with disabilities were treated in university settings. They began wondering what that history was at UConn.
Over the course of roughly 400 hours going through documents in the archives, the professor and her students unearthed a story of an institution that reflected the shifts and changes in contemporary opinions about the proper setting and treatment for people with intellectual disabilities.
The site was a hospital in the mid-1800s and a labor farm in the 1920s. By the 1960s, it was the site of psychological experimentation. In subsequent decades, treatment for the resident population transformed from restraint, seclusion and the use of heavy sedatives to more modern care — such as homier living quarters and more targeted pharmaceuticals.
Over the years, its barracks-style residences, cut off from society at large, were replaced with smaller dormitories and more integrated living — group homes — in the surrounding community. Ultimately, in 1993, shifting public opinion and legal battles put an end to the institution all together.
Continued
| |
He Died at a School for Disabled People. Decades Later, His Brother Sought Answers.
By Sonia A Rao, The New York Times, November 12, 2025
David Scott rose around 7 a.m. that day, as he did every day, and helped his son Michael get dressed and into his wheelchair. Then he found some free time to look at his phone.
It was March 2021. Sitting on his bed in Brockton, Mass., he typed in a search for the “Fernald school,” the state school for disabled people where his oldest brother, John, had lived and died decades earlier.
John’s name had rarely been spoken of in the Scotts’ household. To Mr. Scott, he was more of a specter than a brother. Now retired, Mr. Scott had questions, and time to look for answers.
He tapped on a link. Someone had listed the names of a few hundred people buried in unmarked graves near the Fernald campus. Mr. Scott swiped through the roster.
Ralph R. O’Connell. Gertrude Willwerth.
His fingers stilled. John Scott. C-154.
Finally, he knew where John was. Now he needed to know who he was. It would take three years, the generous help of a local historian and a personal appeal to the governor to find out.
Surrendering John
John Scott was paralyzed in both legs when he was born in June 1955. He had a severe form of spina bifida, a condition in which the spine and the spinal cord don’t form properly. At 18 days old, he was admitted to the Walter E. Fernald State School in Waltham, Mass.
The Fernald, as many locals refer to it, was one of hundreds of public institutions across the country for people with intellectual and developmental disabilities. At their peak in the mid-20th century, these institutions held hundreds of thousands of people, some all but forgotten by their families. After reports of widespread abuses and an outcry from disability rights advocates, most of them were shuttered.
Continued
| | |
Please share this offer with your loved one's
Direct Support Professionals!
VOR ❤️s OUR
DIRECT SUPPORT PROFESSIONALS!
Our loved ones' caregivers are essential to their health, safety, and happiness.
In appreciation of their good work and kind hearts, VOR offers free digital memberships to any DSP who would like to receive our newsletter.
We encourage our members to speak with their loved ones' caregivers to extend this offer of our gratitude.
If you are a Direct Support Professional interested in receiving our newsletter and e-content, please write us at
info@vor.net
with your name, email address, and the name of the facility at which you work. Please include the name of the VOR member who told you of this offer.
| | |
[Please click on blue link to view information about the bill]
VOR SUPPORTS:
H.R.4796 - Rep. Laura Friedman (D-CA) - Restoring Essential Healthcare Act -To amend Public Law 119-21 (The One Big Beautiful Bill Act) to repeal the prohibition on making payments under the Medicaid program to certain entities.
H.R.4807 - Rep Greg Landsman (D-OH) - Protect Our Hospitals Act - To amend Public Law 119-21 to repeal certain changes to provider taxes under the Medicaid program.
H.R.1262 & S.932 - Rep. Michael McCaul (R-TX) and Sen. Markwayne Mullin (R-OK) "Give Kids A Chance Act" - To amend the Federal Food, Drug, and Cosmetic Act with respect to molecularly targeted pediatric cancer investigations. This bill would renew research into pediatric cancers and includes increasing funding for rare diseases, some of which cause Intellual and developmental disabilities and autism.
H.R.1509 & S.752 - Rep. Lori Trahan (D-MA) & Sen. Chuck Grassley (R-IA)
Accelerating Kids' Access to Care Act -
This bill would amend titles XIX and XXI of the Social Security Act to streamline the enrollment process for eligible out-of-state providers under Medicaid and CHIP, and streamline enrollment under the Medicaid program of certain providers across State lines.
H.R.2598 & S.1277 - Rep Jared Huffman (D-CA) and Sen Chris Van Hollen (D-MD) The IDEA Full Funding Act
To amend part B of the Individuals with Disabilities Education Act to provide full Federal funding of such part.
S.2279 - Sen. Josh Hawley (R-MO)
A bill to repeal the changes to Medicaid State provider tax authority and State directed payments made by the One Big Beautiful Bill Act and provide increased funding for the rural health transformation program.
H.R.1950 - Rep. Mark Pocan (D-WI) - Protect Social Security and Medicare Act
To protect benefits provided under Social Security, Medicare, and any other program of benefits administered by the Social Security Administration or the Centers for Medicare and Medicaid Services.
S.779 & H.R.1735 - Sen. Alex Padilla (D-CA) & Rep. August Pfluger (R-TX)
To amend title XIX of the Public Health Service Act to provide for prevention and early intervention services under the Block Grants for Community Mental Health Services program
H.R.2491 & S.1227 - Rep Kat Cammack (R-FL) & Sen. Edward Markey (D-MA) - The ABC Act
To require the Administrator of the Centers for Medicare & Medicaid Services and the Commissioner of Social Security to review and simplify the processes, procedures, forms, and communications for family caregivers to assist individuals in establishing eligibility for, enrolling in, and maintaining and utilizing coverage and benefits under the Medicare, Medicaid, CHIP, and Social Security programs
VOR OPPOSES:
H.R.2743 & S.1332 - Rep. Bobby Scott (D-VA) & Sen. Bernie Sanders (I-VT) Raise the Wage Act - A bill to provide increases to the Federal minimum wage and for other purposes. VOR opposes the provision in this bill that would phase out section 14(c) and sheltered workshops for indiviiduals with I/DD and autism.
S.2438 - Transformation to Competitive Employment Act (Sen. Chris Van Hollen (D-MD) - A bill to assist employers providing employment under special certificates issued under section 14(c) of the Fair Labor Standards Act of 1938 in transforming their business and program models to models that support people with disabilities through competitive integrated employment, to phase out the use of such special certificates, and for other purposes.
| |
836 South Arlington Heights Road #351
Elk Grove Village, IL 60007
Toll Free: 877-399-4867 Fax: 877-866-8377
| | FACEBOOK: /VOR ----- TWITTER: @VOR_NET ----- YouTube | | | | |