|
VOR's Weekly News Update
VOR is a national non-profit organization
run by families of people with I/DD and autism
for families of people with I/DD and autism.
| | |
VOR's Annual Fall Fundraising Campaign!
This is the most important time of year for our fundraising.
Most of our membership renewals and donations
will come in the next three months.
So this is when we start gathering our nuts for the Winter.
| | |
It's Make-It-Or-Break-It Season for VOR.
Over the next two and a half months, we promise to send you a multitude of reasons to donate, to renew your membership, to make end-of-year tax deductions,
to Give us a Tuesday, remember our families during the holidays, share with you the joys and sorrows that bring us together for this important, important cause and to celebrate the good work we do together!
We will try to make our campaigns enjoyable, interesting, touching, and inspiring.
| | |
The Autumn Edition of the VOR Voice
is now available on our website
| | |
VOR's Fall / Winter Fundraising Campaign:
Express your gratitude to the
Direct Support Professionals
in your life
with a little something extra this year...
| | |
Once again, we have partnered with See's Candies in our 2025 Year-End Fundraising Campaign.
See's has agreed to give us a share of the profits for each box sold.
The idea is not to replace our regular appeal for donations,
but to enhance our fundraising efforts by offering delicious See's Candies to our folks who wish to send gifts to family and friends over the holidays.
You may start ordering now.
Candy will begin shipping on November 10, 2025
The last day to order is December 5, 2025
~~ Free Shipping on all orders over $75 ~~
(Except to PO Boxes as extra packaging is required)
| | |
Hosted by Casey Henry and Brenna Redfearn
on our YouTube page!
| | Our Dysfunctional Government: | |
Government Shutdown Has Disability Providers ‘Running On Fumes’
By Michelle Diament, Disability Scoop, October 28, 2025
Nearly a month into the federal shutdown, some organizations aiding people with disabilities are starting to scale back services as the effects begin to mount.
The government shut down at the beginning of the month when Congress failed to agree on spending before the start of the new fiscal year. Since then, thousands of workers have been furloughed and federal agencies have only operated services deemed essential.
Social Security and Supplemental Security Income payments and funding for Medicaid home and community-based services have continued, but other operations including civil rights investigations at the U.S. Department of Education are at a standstill. Military families have reportedly seen coverage of applied behavior analysis therapy for their children with autism halted and at least one state-run job training program for people with disabilities — the Tennessee Rehabilitation Center-Smyrna — closed its doors as a result of the shutdown.
Now, protection and advocacy organizations — which exist in each state to provide free legal and advocacy services to individuals with disabilities — are feeling the pinch.
In what may be the most extreme example, Disability Rights Arkansas said last week that it would stop taking new cases and the organization plans to furlough staff beginning Nov. 1 citing “unprecedented funding challenges” stemming from the shutdown.
“We have been operating on limited carryover funds from FY 2025, which are now nearly exhausted,” Tom M. Masseau, the group’s executive director, said in a statement. “Without new federal funding, we are forced to make difficult decisions to preserve our ability to serve existing clients and maintain core operations.”
Masseau told Disability Scoop that funding for two of the organization’s nine grants are out of money and two more will be depleted by mid-November.
“The longer the shutdown goes on, the more difficult decisions I will have to make around the holidays,” he said.
There’s also growing concern about what’s to come, said Maria Town, president and CEO of the American Association of People with Disabilities. Federal funding for the Supplemental Nutrition Assistance Program, which provides food aid and is disproportionately relied on by people with disabilities, is set to run out by the end of the month and new Section 8 housing vouchers will not be issued after November if a deal isn’t reached, she said.
“Given how many people with disabilities rely on benefits from government programs, this shutdown is especially harmful for the disability community,” Town said. “We know that the longer the shutdown lasts, the more we can expect disruptions in administrative work and delays in services, including the processing of disability benefits applications and Medicaid/Medicare claims. It is crucial for lawmakers to reach a deal to fund the government.”
Read the full article here
| | |
Breaking News:
Two judges rule Trump admin must keep SNAP benefits in place as shutdown drags on
By Breanne Deppisch, Fox News, October 31, 2025
A federal judge on Friday ordered the Trump administration to continue to fund Supplemental Nutrition Assistance Program (SNAP) during the ongoing government shutdown, delivering near-term relief to roughly 42 million Americans who received the aid just hours before the funding was slated to dry up.
The emergency order from U.S. District Judge Indira Talwani said the Trump administration must resume SNAP benefits, which were slated to expire Nov. 1, ruling that plaintiffs who filed the lawsuit are likely to succeed on their claims that the suspension of the benefits is unlawful. She ordered the government to provide the court no later than Monday, Nov. 3, with additional details on how it plans to keep the program funded, and whether the appropriated benefits must be distributed in full or in part.
Moments later, a separate federal judge in Rhode Island ordered the Trump administration to continue paying for food stamps during the shutdown.
U.S. District Judge John McConnell said the administration must tap its emergency funds to pay for the SNAP benefits "as soon as possible" next month. He issued the emergency order from the bench Friday during an emergency court hearing in Providence.
Talwani heard arguments Thursday from the Trump administration and from a coalition of 25 Democratic governors and state attorneys general, who sued the U.S. Department of Agriculture over its refusal to keep SNAP benefits funded during the ongoing government shutdown.
The benefits were slated to expire Nov. 1, marking the first time in 60 years that the program lapsed because of a government shutdown.
Talwani seemed sympathetic to the states’ arguments on Thursday. "It’s hard for me to understand how this isn’t an emergency when there’s no money and a lot of people need their SNAP benefits," she said in court, vowing to rule as soon as possible on the matter.
She also agreed with the argument that the cuts to SNAP would be "devastating."
State leaders said in the lawsuit that suspending the aid would disproportionately harm some tens of millions of vulnerable and low-income Americans in their states. "Because of USDA’s actions, SNAP benefits will be delayed for the first time since the program’s inception," they said in the lawsuit, filed Tuesday.
"Worse still, USDA suspended SNAP benefits even though, on information and belief, it has funds available to it that are sufficient to fund all, or at least a substantial portion, of November SNAP benefits," they added.
Read the full article here
| |
Disability services staffing squeezed as Medicaid cuts loom
By Maya Goldman, Axios, October 29, 2025
Nearly 90% of the organizations providing Medicaid-funded community services for people with intellectual or developmental disabilities had staffing shortages this year, according to a trade group for the providers.
Why it matters: Staffing already is a long-standing problem for disability services providers and is expected to get worse as the effects of the budget reconciliation law and its nearly $1 trillion in Medicaid cuts are felt.
- State Medicaid programs aren't required to cover home- and community-based services and have cut funding in the past to respond to budget constraints.
State of play: More than 60% of 469 providers surveyed by the trade group ANCOR in August and September said they've had to turn away referrals of new program participants due to lack of staff.
- "Long-term underinvestment in Medicaid has hamstrung community providers' ability to offer wages that are competitive with employers in hourly wage industries, such as retail and fast food," ANCOR wrote in a report on its survey provided first to Axios.
- "Now, we see clearly the profound impact of these dynamics on the ability of community providers to deliver essential programs and support people with disabilities in their homes and communities."
Friction point: People with intellectual and developmental disabilities spent an average of 50 months on waitlists for Medicaid home- and community-based care services last year, per KFF.
- If providers don't have enough staff, people have to forgo services or stay in hospitals or institutional settings for longer, ANCOR said.
- Some states require people to access services within a certain time after coming off the waitlist. If no provider is available, they could end up back on the waitlist, according to the report.
Zoom in: Some 29% of providers report discontinuing services this year — lower than last year's 39%.
- But 52% reported considering additional cuts to programs, compared with 34% in 2024.
- Providers this year were most likely to report cutting back on residential services including around-the-clock at-home support and hourly skill-building and socialization support.
Read the full article here
Download ANCOR's report here
| |
Family Caregivers Struggling In Some States More Than Others
By Shaun Heasley, Disability Scoop, October 31, 2025
Nearly a quarter of U.S. adults provide care to loved ones with disabilities or complex medical conditions, but a new report finds that the challenges they face vary significantly depending on which state they call home.
State policies on paid leave, respite care and other factors are dramatically impacting the reality of these family caregivers, according to the report out this week from AARP and the National Alliance for Caregiving.
Across the country, there are an estimated 63 million family caregivers, but they are not distributed evenly. The share of adults serving in this role varies from 20% in Washington, D.C. to 34% in Mississippi, the data shows.
Among family caregivers, 18% are paid for some of the support they provide, often through Medicaid home and community-based services self-direction waivers or other government programs. State-level data, however, reveals wide discrepancies, with just 10% of family caregivers in Iowa receiving pay versus a high of 28% in New Jersey.
“These state-by-state disparities expose how policy choices determine whether families thrive or collapse under caregiving responsibilities,” said Jason Resendez, president and CEO of the National Alliance for Caregiving. “When financial strain hits 59% of family caregivers in Georgia compared to just 34% in Minnesota — meaning where you live can double your risk of economic hardship — it’s clear that patchwork state solutions aren’t enough.”
Two-thirds of family caregivers assist with at least one task considered an activity of daily living like bathing, dressing, feeding or toileting and virtually all of them help with financial management, shopping or other tasks necessary for independent living, according to the report.
Almost half of family caregivers are engaged in high-intensity care and 28% provide 40 or more hours of care each week. Tennessee has the largest share of caregivers putting in this number of hours at 37%, the report found.
These responsibilities are leading to financial and health consequences for family caregivers, with many struggling to find affordable local services for the person they assist or facing difficulty caring for their own health, the findings show.
Read the full article here
Download the report from AARP and the National Alliance for Caregiving here
| | |
Who qualifies for Medicaid coverage?
The Medical Frailty Exemption: The Implementation Cornerstone of Medicaid Work Requirements
By Patti Boozang and Kinda Serafi, The 80 Million, October 29, 2025
- Congress sought to protect vulnerable individuals from losing coverage by expressly exempting medically frail individuals from work requirements. In doing so, H.R.1 provides for minimum standards for individuals who are medically frail, meaning they experience serious physical and intellectual disabilities, complex medical conditions, behavioral health problems, and/or a substance use disorder.
- Historically, the Centers for Medicare & Medicaid Services (CMS) has deferred to states to define medical frailty — a definition that will matter a great deal for Americans who may qualify for exemptions from the forthcoming Medicaid work reporting requirements that will take effect Jan. 1, 2027.
- Defining medical frailty, and determining who qualifies for such exemptions, is another important task added to states’ growing list of action items as new policies implemented under H.R.1 begin to take effect. Manatt toolkits for the State Health & Value Strategies (SHVS) program provide a strong start to the work.
-
Ex parte data verification is required to identify medically frail individuals and will be essential to states’ medical frailty exemption processes. Simple, straightforward and accessible application screening questions will also help new applicants self-identify as medically frail.
As states prepare for the Jan. 1, 2027, implementation of federally mandated Medicaid work reporting requirements, the most consequential — and complex — decisions lie in how states define and operationalize the medical frailty exemption. Defining “medical frailty” and building systems and operational capacity to identify and verify those medical conditions are proving to be one of the most challenging aspects of implementation for states. Specifically, states will need to build new operational processes and IT systems that bridge claims, encounter and other data with their eligibility and enrollment system in order to exempt individuals identified as medically frail.
Under H.R.1, individuals who are “medically frail or otherwise have special medical needs” are exempt from Medicaid work reporting requirements. The statute provides a floor — not a ceiling — for qualification:
- Individuals with a substance use disorder
- Those with disabling mental disorders
- People with significant physical, intellectual or developmental disabilities that impair daily functioning
- Individuals with a serious or complex medical condition
- Those who are blind or meet the Social Security Administration (SSA) definition of disability
States have flexibility to define which diagnoses and types of services fall within these categories. It’s essential that they do so within a framework that is operationally feasible, data-driven, and ensures applicants and enrollees are able to access the pathways to exemption if they are eligible.
Defining Medical Frailty
Manatt Health, through the Robert Wood Johnson Foundation-funded SHVS program, has developed a suite of toolkits to support states in implementing work requirements in a manner that ensures that eligible people get and stay enrolled in Medicaid. These toolkits establish implementation planning milestones to support states’ work planning, lay out key policy and operational decision points, tee up potential data verification processes for verifying compliance and exemptions and coordinating with the Supplemental Nutrition Assistance Program, and offer considerations for states as they develop a strategic verification hierarchy for work requirements exemptions and compliance.
Most recently, Manatt Health released a medical frailty toolkit that provides a description of the factors that states may consider when developing medical frailty definitions, examples of potential state definitions, and the types of claims data diagnosis and utilization codes that states can used to assess and verify medical frailty. States (as well as vendors and other stakeholders) can use this toolkit as a jumping off point for developing sound, inclusive definitions and data verification strategies.
Data Is the Backbone of Medical Frailty Determination
Ex parte verification — using data sources to confirm exemption status without requiring additional documentation from enrollees — is not just a best practice, it’s a statutory requirement under H.R.1 and will be critical in identifying people who are medically frail and should be exempt from work requirements. Leveraging claims, encounter data and other new data sources is a key component to identifying individuals who meet the medically frail definition. To do that, states will need to develop a code list of diagnoses, service utilization, pharmacy and durable medical equipment that align with the states’ definitions of medical frailty that will be used to data mine Medicaid Management Information Systems. States can also identify medically frail individuals who are assigned to a state program where eligibility aligns with medical frailty (e.g., a behavioral health managed care plan) and through information provided by a managed care plan based on utilization data review and information provided by care managers. By leveraging new and existing datasets, states can verify whether enrollees qualify for the exemption. Absent reliance on data, the burden of proof for exemption falls to individuals, and experience tells us they are likely to fail in demonstrating their medical frailty.
Getting the data sources and systems in place will be a heavy lift for states, especially as they race to implement their work reporting requirement technology by January 2027. Most states, if not all, will need to build or enhance data-sharing infrastructure, develop new algorithms to flag potentially frail individuals, and train eligibility workers and managed care organizations on how to interpret and act on these data.
The Bottom Line
If states stumble in their decision making and execution around medical frailty exemption policy, systems or operations, the consequences can be severe. Medically frail individuals could be denied or lose coverage, leading to disenrollment, worsening health and increased costs down the line for the Medicaid program. But if states get it right, they can make data informed, person-centered medical frailty exemption decisions, protecting the most vulnerable people in the program and meeting the intent of the mandatory eligibility condition established by Congress. The clock is ticking to get it right.
Read the full article here
| |
Officials Show Little Proof That New Tech Will Help Medicaid Enrollees Meet Work Rules
By Rae Ellen Bichell and Sam Whitehead, KFF Health News, October 23, 2025
This summer, the state of Louisiana texted just over 13,000 people enrolled in its Medicaid program with a link to a website where they could confirm their incomes.
The texts were part of a pilot run to test technology the Trump administration says will make it easier for some Medicaid enrollees to prove they meet new requirements — working, studying, job training, or volunteering at least 80 hours a month — set to take effect in just over a year.
But only 894 people completed the quarterly wage check, or just under 7% of enrollees who got the text, according to Drew Maranto, undersecretary for the Louisiana Department of Health.
“We’re hoping to get more to opt in,” Maranto said. “We plan to raise awareness.”
The clock is ticking for officials in 42 states — excluding those that did not expand Medicaid at all — and Washington, D.C., to figure out how to verify that an estimated 18.5 million Medicaid enrollees meet rules included in President Donald Trump’s tax and spending law. They have until the end of next year, and federal officials are giving those jurisdictions a total of $200 million to do so.
The policy change is one of several to free up money for Trump’s priorities, such as increased border security and tax breaks that mainly benefit the wealthy.
The nonpartisan Congressional Budget Office has said the work rules will be the main reason millions of people won’t be able to access health insurance over the next decade. It estimates changes to the Medicaid program will result in 10 million fewer Americans covered by 2034 — more than half of them because of the eligibility rules.
For now, state officials, health policy researchers, and consumer advocates are watching the pilot program in Louisiana and another in Arizona. Mehmet Oz, director of the Centers for Medicare & Medicaid Services, has touted those test-drives and said they will allow people to verify their incomes “within seven minutes.”
“There have been efforts to do this in the past, but they haven’t been able to achieve what we can achieve because we have technologies now,” said Oz, during a television appearance in August.
Brian Blase, the president of the conservative Paragon Health Institute and a key architect of Medicaid changes in the new law, has chimed in, saying during a recent radio appearance that with today’s artificial intelligence “people should be able to seamlessly enter how they are spending their time.”
KFF Health News found scant evidence to support such claims. Federal and state officials have offered little insight into what new technology the two pilots have tested. They do say, however, that it connects directly with the websites of Medicaid enrollees’ payroll providers, rather than using artificial intelligence to draw conclusions about their activities.
Officials have also offered few details about the pilots’ effectiveness in assisting enrollees in Medicaid or other public benefit programs.
The shortage of information has some state officials and health policy researchers worried that the Trump administration lacks viable solutions to help states implement the work rules. As a result, they say, people with a legal right to Medicaid benefits could lose access to them.
Read the full article here
| | Intellectual Disabilities and Mental Illnesses: | |
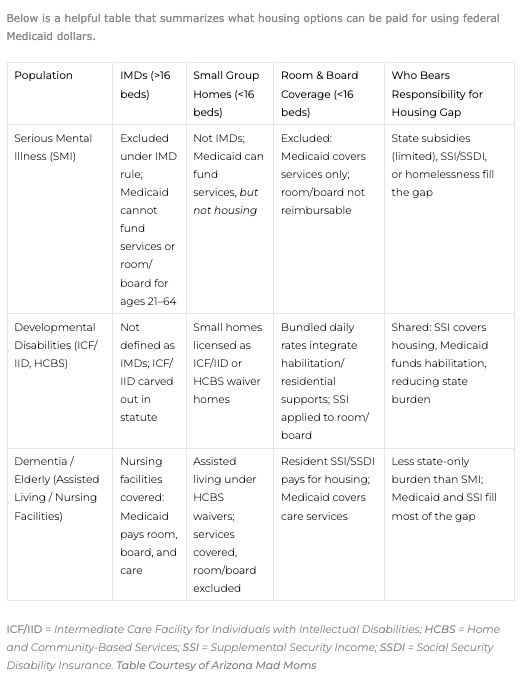
What’s the IMD Exclusion? Why is the Exclusion a Barrier to Housing People with a Serious Mental Illness?
By Rachel Streiff and Will Humble, Arizona Public Health Association, October 27, 2025
Have you ever wondered why most US states have so many homeless individuals with severe mental illnesses? Perhaps you have noticed a stark contrast to other disabled populations, such as those with developmental, physical or elderly disabilities. While services may not be perfect for these other vulnerable populations, they’re still, generally, housed.
AHCCCS’ last report showed more than 6,000 Arizonans formally designated with a Serious Mental Illness (SMI) on a waiting list for housing. Yet, the Arizona Long Term Care System (ALTCS) for both the Elderly and Physically Disabled (EPD) and Division of Developmental Disabilities (DDD) populations report relatively few on their housing waitlists; generally less than couple hundred such individuals are “in between” placements.
Arizona’s Medicaid system has a unique entitlement program that covers SMI treatment, offering a range of short-term services including inpatient hospitals and Behavioral Health Residential Facilities (BHRF’s).
Yet there are scant few housing options once they are discharged. More fortunate individuals may go home to a family caregiver, or to the scarce network of SMI supported housing units. Those less fortunate find themselves on streets, in shelters, in carceral settings, or worse: the morgue. I have extensively reported on the deadly combination of SMI, homelessness, and the Arizona heat.
The enormous housing gap uniquely affecting the SMI population is a direct result of the “IMD exclusion.” Perhaps you’ve heard of it but aren’t sure what it is and what it’s doing.
What’s the IMD Exclusion?
Medicaid was set up in 1965 under the Social Security Act. It included a provision called the Institution for Mental Diseases (IMD) exclusion which banned federal funds from being used for treatment in psychiatric facilities with more than 16 beds. The goal was to stop federal funding of state asylums which had few care standards, no oversight, and were notorious for indefinitely warehousing people with disabilities, including SMI.
This kicked off a movement known as “Deinstitutionalization.” States were de-incentivized to institutionalize people and were expected to create mental health systems that provided treatment in their communities.
Over time, advances in medicine and law made institutionalization far less likely. Psychiatric and medical inpatient admissions criteria were set up, as well as legal criteria needed to justify involuntary treatment. Medications like antipsychotics became increasingly more effective.
Despite these advances, certain conditions like Schizophrenia still had a subset of individuals that needed a higher level of care to keep stability and safety. Eventually, the IMD exclusion caused major unintended consequences for this chronic SMI population – not just by restricting access to hospitals, but also by cutting off pathways to permanent housing for many people with SMI.
Both ALTCS populations (EPD and DDD) have not faced chronic homelessness in the same way. This is because, almost since its start, Medicaid provided funding for Intermediate Care Facilities (ICFs) serving individuals with intellectual disabilities. Then in 1981, Congress added the Home and Community-Based Services (HCBS) waiver.
This allowed state Medicaid programs to cover long-term care for individuals with intellectual and developmental disabilities (IDD) outside of institutional settings, in homes and group homes.
These same Long-Term Support Services were extended to the EPD population, since their conditions were defined as physical or medical rather than “mental diseases.” This allowed skilled nursing facilities — and later HCBS programs — to use federal Medicaid dollars for residential care.
These “ exceptions” to the IMD exclusion made Medicaid housing coverage possible for certain disabled populations: if you are eligible for a Medicaid-funded institution, Medicaid can pay for you to live in a home or group home instead. By contrast, a comparable waiver was never created for the SMI population.
The IMD exclusion serves to double-down on Congress’s stance that individuals living with mental illness ought not to receive the long-term care benefits provided to the IDD and EPD populations.
| |
Instead of being reintegrated into supported community residential settings, people with SMI were often deinstitutionalized into homelessness, jails, and prisons — a process known as trans institutionalization.
The IMD exclusion, meant to prevent warehousing in large, locked hospitals, evolved into a blanket ban on Medicaid’s participation in almost ALL housing for adults with SMI—even small, unlocked, community-based group homes with fewer than 16 beds.
Without federal help, state budgets must cover the SMI housing gap, and most states fall short. Although the Olmstead decision mandated that states provide disabled people with appropriate community-based settings, it does not override Medicaid’s funding restrictions.
Read the full article here
| |
Strengthening the Respite Care Workforce
By Kimberly Hodges and Wendy Fox-Grage, National Academy for State Health Policy, October 30, 2025
The Workforce Behind the Care
Family caregivers often say what they most need is a break. Respite care — for example, provided by aides who can provide temporary, intermittent care or by adult day centers — can give families this needed break. The big problem is finding a well-qualified workforce that can provide the care.
The fundamental challenges facing the respite care workforce mirror those of the broader direct care workforce. Despite being one of the fastest-growing sectors in the U.S. — driven largely by an aging population — respite care providers and the direct care workforce often face low wages, limited career advancement opportunities, and inadequate training and supervision. These systemic issues hinder recruitment and retention, ultimately affecting the quality and availability of care.
At the session, subject matter experts emphasized the need to break down silos between respite care providers and the broader direct care workforce such as personal care and home care aides. Rather than treating these as separate entities, there is an opportunity to create unified career pathways and matching service registries that allow individuals to move fluidly between roles and advance in their career path, enhancing both workforce flexibility and career development.
National Respite Care Provider Training
The NRCPT, in part funded by the U.S. Administration for Community Living, is a free, online, self-paced entry-level curriculum centered on 10 core competencies and consists of 10 courses. This training is designed to be accessible in a variety of settings, with materials available in English and Spanish. It is structured to support both the paid workforce and volunteers (i.e., family and friends of caregivers) who have never provided respite or would like to refine their skills. The training can serve as a foundational step in a broader career ladder. The training is replicable and scalable by a replication toolkit to facilitate state-specific adoption.
Ten sites across the U.S. tested the training curriculum and a specialized respite provider recruitment campaign during a 12-month pilot. After positive results, many of them are continuing to use the curriculum after the pilot testing period.
Final evaluation results show that learners reported improved confidence in respite provider core competencies. Most learners were new to respite (62 percent), lived in small towns (population between 2,500 and 49,000 people) (40 percent) or rural communities (population less than 2,500 people) (23 percent), and indicated they are very likely (67 percent) to provide respite in the next six months. Key lessons from the pilot included the importance of marketing the training as a recruitment tool, forming partnerships to support outreach and recruitment, and connecting trained providers to respite opportunities through registries and other platforms.
Workforce Registries and Training: Lessons from North Dakota and Wisconsin
Direct support workforce registries are online platforms that connect people needing care to qualified service providers. The types of workers listed on a registry can include job titles such as home care worker, home health aide, personal care attendant, and direct support professional, among others. According to data from PHI, 12 states operate regional or statewide matching service registries. Similarly, respite registries connect both the care recipient and their caregiver to a qualified respite provider.
North Dakota: North Dakota’s Qualified Service Provider (QSP) and QSP Agencies Public Registry includes a wide range of service providers — not just those offering respite care. It captures essential information such as service type, contact details, agency affiliation, personal preferences, and geographic location. A standout feature of North Dakota’s registry is its real-time updating system. Providers enroll through a dedicated portal, and an interface feeds information into the registry to ensure updates are reflected daily. This commitment to accuracy enhances the registry’s reliability and usability for care recipients and family caregivers. Through the NASHP learning collaborative, the state is exploring the use of the National Respite Care Provider Training and integrating it into the registry platform.
Wisconsin: The Wisconsin Respite Care Registry offers family caregivers the ability to search for respite care providers that offer in-home and facility-based respite. Respite Care Association of Wisconsin (RCAW) created the National Respite Care Provider Training and administers the respite care provider registry for the state. RCAW is funded by state general revenue and some federal grant funding. Both independent respite providers and provider agencies can create a user-friendly profile on the registry, including a short biography, which orients potential caregivers and care recipients to a more personalized introduction to the provider.
Providers from Wisconsin that have completed the National Respite Care Provider Training are integrated into the registry. The registry also includes strong disclaimer language clarifying that it does not guarantee care connections, emphasizing that RCAW is not the employer and the need for individuals to vet providers independently. The Wisconsin Department of Justice’s Wisconsin Online Record Check System can conduct a background check on behalf of the caregiver for a small fee. The registry is limited to respite care providers rather than the broader direct care workforce. Conversely, family caregivers can also post their caregiving needs on Respite Connections, acting as a reverse registry.
Conclusion
The direct care workforce is one of the fastest growing occupations in the U.S. — with statistics showcasing a projected 772,000 new jobs by 2034. Respite care providers are integral to the overall workforce as they provide caregivers a much-needed break. As an emerging innovation from NASHP’s Caregiving State Policy Learning Collaborative, state governments have made investments in supporting family caregivers — including the provision of respite care. Research has found that when older adults’ caregivers receive supports that include respite, caregiver outcomes improve, older adults’ nursing home placement is delayed, and hospital readmissions and emergency room expenditures are decreased. The insights shared in this paper offer states examples to strengthen their respite care workforce to help ensure that caregivers have access to high-quality respite care.
Read the full article here
| |
NJ's health sytem has a huge gap in care for people with disabilities on Medicaid
By Scott Fallon and Gene Myers, North Jersey .com, October 30, 2025
When Nantanee Koppstein found a new primary care practice in the Princeton area for her daughter, she was overjoyed — considering that it took weeks of searching for a doctor who had experience treating a patient with developmental disabilities.
The first visit was great. The doctor was kind and competent. Koppstein and her daughter, who has multiple disabilities, were confident they had found a practice that would serve them for years.
But a few weeks later, in early 2020, Koppstein's hopes came crashing down.
The practice informed Koppstein that they could no longer see her daughter because she was on Medicaid — even though it was not her primary insurance.
“I called the administrators and practically begged them to reconsider,” Koppstein said. "But it’s like a red flag goes up everywhere whenever they see Medicaid.”
In a state known for its social safety net and one of the best doctor-to-patient ratios in the nation, New Jersey has historically sat at the bottom of an important list that runs counter to both factors.
The Garden State has long had one of the lowest Medicaid reimbursement rates in the U.S., resulting for years in the lowest percentage of doctors who accept new Medicaid patients — government health insurance for low-income residents and for many with disabilities.
State officials said they have made strides in recent years to increase the number of providers who take Medicaid.
But the low percentages over the years have created a huge gap in care, especially for tens of thousands of patients with developmental and intellectual disabilities when they age out of their parents’ private insurance coverage and into Medicaid.
For patients with disabilities, finding a primary care doctor or specialist who can take care of their needs is hard enough. Finding one who will also take their low-paying government insurance is even more difficult.
Continued
| |
North Carolina families, caregivers report widespread impact from Medicaid cuts
By Matthew Ablon, WCNC News, October 30, 2025
Medicaid cuts are disrupting services for North Carolina residents with intellectual and developmental disabilities, forcing wage reductions for caregivers and threatening the stability of community-based support programs, according to a new report from the North Carolina Council on Developmental Disabilities.
The council surveyed 345 individuals between Oct. 1 and Oct. 18, collecting responses from family caregivers, people with disabilities, direct support professionals, and service providers. The report, released Thursday, details immediate financial impacts and growing concerns about the sustainability of home and community-based care.
Direct support professionals reported wage cuts ranging from 3% to 10%. One paid caregiver, who works 36 to 40 hours weekly caring for a medically fragile child, said their pay was cut by 8%.
"I can't afford to get a second job, and I don't want to leave this family," the caregiver wrote in the survey.
The report identifies a workforce crisis, with providers struggling to compete with retail employers. One Asheville provider said a direct support professional candidate declined a position because she earns $23 per hour at Sam's Club.
Respondents reported disabilities including autism spectrum disorder, cerebral palsy, epilepsy, and genetic disorders such as Down syndrome and Fragile X. Many individuals have multiple co-occurring conditions requiring complex care.
Families said they rely on Medicaid-funded services, including the Innovations Waiver, therapy services, respite care, and community living supports. One parent said their family waited 11 years for the Innovations Waiver.
Some agencies are considering layoffs, property sales, or closures. One provider said the organization is looking at selling a thrift store to maintain day services.
Continued
| |
Cuts to Medicaid have already begun to leave their mark in Virginia
Bu Mackenzie Konjoyan, The Virginia Independent, October 30, 2025
Elena Hung is the mother of a girl she calls a “medically complex” child. For the first five months of her life, Hung’s daughter Xiomara was in the neonatal intensive care unit of a hospital. Their medical bill was over $3 million.
Hung’s health insurance covered the costs of extended hospital stays, but it didn’t cover the home and community-based services Xiomara, who has a tracheostomy to breathe and a feeding tube for all of her nutrition, needed to remain medically safe at home.
“Even with that private insurance, it still did not cover everything she needed — not even close — and we had to rely on Medicaid,” said Hung, a co-founder and the executive director of the group Little Lobbyists, which advocates for children with complex medical issues and disabilities.
Hung said a Medicaid waiver covers the costs of the trained nurse her daughter needs to help her attend public school. Medicaid allows Xiomara to live at home with her family and receive the therapies that allow her greater independence.
Waivers, which in Virginia include Developmental Disability and Commonwealth Coordinated Care Plus waivers, allow Medicaid to cover services that otherwise would not be reimbursed under federal law, such as home and community-based services. Those with Medicaid waivers might have longer waiting lists or receive fewer resources dedicated to their needs due to funding changes and cuts included in President Donald Trump’s One Big Beautiful Bill Act, reported the health policy research organization KFF.
Losing Medicaid waivers that cover home-based care would mean Hung’s daughter and other medically complex children would face the immediate risk of having to live in a medical facility, away from their families.
“Without Medicaid, children like mine don’t get to have a life — don’t get to have quality of life, but don’t get to have a life. If she doesn’t have the support she needs, she’s not medically safe,” Hung said.
KFF said that with the passage of the H.R.1 in July, the Congressional Budget Office has projected that the number of uninsured people could increase by as many as 5.3 million by 2034 under new Medicaid eligibility requirements.
Continued
| |
Despite Hold On Ed Department Layoffs, Special Education Worries Run High
By Michelle Diament, Disability Scoop, October 30, 2025
A judge indefinitely blocked the U.S. Department of Education from laying off nearly every staffer in its special education office, but advocates say concerns about the future of the program remain.
At a hearing this week, Judge Susan Illston of the U.S. District Court for the Northern District of California barred federal agencies, including the Education Department, from firing workers during the government shutdown.
The decision comes more than two weeks after the Education Department laid off 121 employees in its Office of Special Education and Rehabilitative Services, leaving no more than a handful of staff in the agency’s Office of Special Education Programs, which administers funding and oversees implementation of the Individuals with Disabilities Education Act. Unions representing many affected workers sued over the job cuts.
In moving to extend a temporary pause issued earlier this month, Illston said she expects to find that the government’s actions to authorize so-called reductions in force, or RIFs, during the shutdown are “unlawful.”
“I believe that I will find that their actions are arbitrary and capricious as shown by the haphazard way in which the RIFs have rolled out and they are intended for the purpose of political retribution,” Illston said.
Illston told the Trump administration not to implement RIF notices issued since the government shutdown began earlier this month and not to issue any new ones.
Disability advocates welcomed the decision to halt the layoffs, but cautioned that the situation remains fraught.
“We are thankful for the role the courts are playing in keeping this horrific decimation from going forward,” said Denise Marshall, CEO of the Council of Parent Attorneys and Advocates, or COPAA, a nonprofit that advocates for the rights of students with disabilities and their families. “We will not relent or be relieved until it’s permanently behind us. The threat remains high for students with disabilities and their families.”
Currently, many federal workers are furloughed due to the shutdown, but per the court order, workers are expected to return to the Education Department’s special education office whenever the government reopens, Marshall said.
However, Stephanie Smith Lee, co-director of policy and advocacy at the National Down Syndrome Congress, who served as director of the Education Department’s Office of Special Education Programs under President George W. Bush, said it is likely that the government will appeal Illston’s decision to block the layoffs.
“If the RIFs are not reversed, OSEP will be unable to fulfill the responsibilities required under the Individuals with Disabilities Education Act (IDEA) even after the shutdown ends,” Lee said. “Without staff to oversee the monitoring and grant programs, or send out funding to the states and centers, services for students with disabilities will erode.”
Continued
| | |
Please share this offer with your loved one's
Direct Support Professionals!
VOR ❤️s OUR
DIRECT SUPPORT PROFESSIONALS!
Our loved ones' caregivers are essential to their health, safety, and happiness.
In appreciation of their good work and kind hearts, VOR offers free digital memberships to any DSP who would like to receive our newsletter.
We encourage our members to speak with their loved ones' caregivers to extend this offer of our gratitude.
If you are a Direct Support Professional interested in receiving our newsletter and e-content, please write us at
info@vor.net
with your name, email address, and the name of the facility at which you work. Please include the name of the VOR member who told you of this offer.
| | |
[Please click on blue link to view information about the bill]
VOR SUPPORTS:
H.R.4796 - Rep. Laura Friedman (D-CA) - Restoring Essential Healthcare Act -To amend Public Law 119-21 (The One Big Beautiful Bill Act) to repeal the prohibition on making payments under the Medicaid program to certain entities.
H.R.4807 - Rep Greg Landsman (D-OH) - Protect Our Hospitals Act - To amend Public Law 119-21 to repeal certain changes to provider taxes under the Medicaid program.
H.R.1262 & S.932 - Rep. Michael McCaul (R-TX) and Sen. Markwayne Mullin (R-OK) "Give Kids A Chance Act" - To amend the Federal Food, Drug, and Cosmetic Act with respect to molecularly targeted pediatric cancer investigations. This bill would renew research into pediatric cancers and includes increasing funding for rare diseases, some of which cause Intellual and developmental disabilities and autism.
H.R.1509 & S.752 - Rep. Lori Trahan (D-MA) & Sen. Chuck Grassley (R-IA)
Accelerating Kids' Access to Care Act -
This bill would amend titles XIX and XXI of the Social Security Act to streamline the enrollment process for eligible out-of-state providers under Medicaid and CHIP, and streamline enrollment under the Medicaid program of certain providers across State lines.
H.R.2598 & S.1277 - Rep Jared Huffman (D-CA) and Sen Chris Van Hollen (D-MD) The IDEA Full Funding Act
To amend part B of the Individuals with Disabilities Education Act to provide full Federal funding of such part.
S.2279 - Sen. Josh Hawley (R-MO)
A bill to repeal the changes to Medicaid State provider tax authority and State directed payments made by the One Big Beautiful Bill Act and provide increased funding for the rural health transformation program.
H.R.1950 - Rep. Mark Pocan (D-WI) - Protect Social Security and Medicare Act
To protect benefits provided under Social Security, Medicare, and any other program of benefits administered by the Social Security Administration or the Centers for Medicare and Medicaid Services.
S.779 & H.R.1735 - Sen. Alex Padilla (D-CA) & Rep. August Pfluger (R-TX)
To amend title XIX of the Public Health Service Act to provide for prevention and early intervention services under the Block Grants for Community Mental Health Services program
H.R.2491 & S.1227 - Rep Kat Cammack (R-FL) & Sen. Edward Markey (D-MA) - The ABC Act
To require the Administrator of the Centers for Medicare & Medicaid Services and the Commissioner of Social Security to review and simplify the processes, procedures, forms, and communications for family caregivers to assist individuals in establishing eligibility for, enrolling in, and maintaining and utilizing coverage and benefits under the Medicare, Medicaid, CHIP, and Social Security programs
VOR OPPOSES:
H.R.2743 & S.1332 - Rep. Bobby Scott (D-VA) & Sen. Bernie Sanders (I-VT) Raise the Wage Act - A bill to provide increases to the Federal minimum wage and for other purposes. VOR opposes the provision in this bill that would phase out section 14(c) and sheltered workshops for indiviiduals with I/DD and autism.
S.2438 - Transformation to Competitive Employment Act (Sen. Chris Van Hollen (D-MD) - A bill to assist employers providing employment under special certificates issued under section 14(c) of the Fair Labor Standards Act of 1938 in transforming their business and program models to models that support people with disabilities through competitive integrated employment, to phase out the use of such special certificates, and for other purposes.
| |
836 South Arlington Heights Road #351
Elk Grove Village, IL 60007
Toll Free: 877-399-4867 Fax: 877-866-8377
| | FACEBOOK: /VOR ----- TWITTER: @VOR_NET ----- YouTube | | | | |