|
The latest doctors' strike fizzles to an end tomorrow.
Forlorn huddles on picket-lines, sheltering from the rain in an arctic blast is not a good look for a profession… neither is singing and cheering.
Picket line etiquette is tricky.
Sir Jim et-al, has managed to keep the show on the road. Amazing!
Streeting continues his performative imitation of a politician.
His lambast, pushing him further away from negotiations and probably not any closer to Downing Street… if you know what I mean.
Let’s stocktake;
-
Public backing for the strikes is declining.
-
Standoff on pay. The BMA demanding pay restoration of roughly ~29%, make up for real-terms losses since 2008.
-
Streeting argues that the recent pay rises total ~28.9% over three years.
-
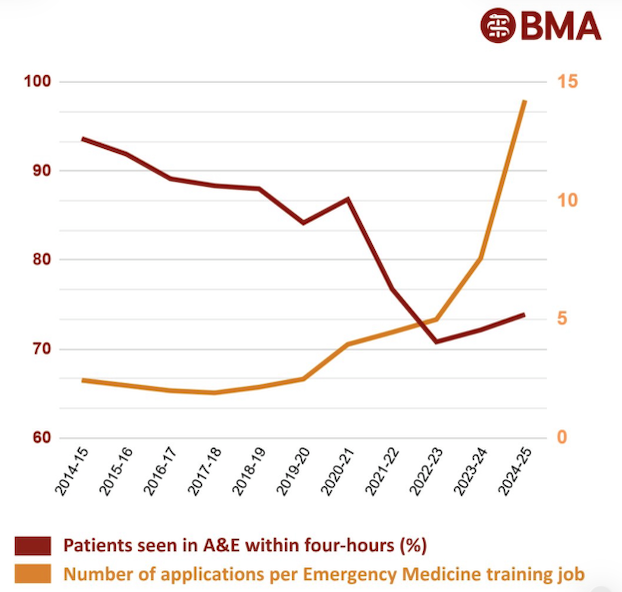
BMA has concerns about career progression (training posts), working conditions and reforms, like exception reporting.
-
Patient trust is eroding. Disrupted services and reform momentum, stalled.
-
There have been meetings… Streeting, has floated non-pay measures ... more training places, loan forgiveness.
What’s next? Well... if I may be so bold…
The BMA...
... has to recognise public support is weakening. That is not good. Acknowledge it and shift messaging from ‘all-or-nothing pay restoration’ to ‘a credible, phased plan.’
It’s no good saying they’re striking for safety and continuity of care and a better NHS. We all know it’s about money and jobs… own it.
Propose and publish a multi-year deal that phases pay restoration, tied to specific milestones… number of training places created, career progression bottlenecks addressed.
Link pay demands to non-pay reforms (which Streeting seems open to). More training, more specialist positions, funding exam or professional fees, better working conditions...
... this reduces the immediate fiscal hit while aligning with doctors’ long-term concerns.
Doctor’s support for strikes is waning. The BMA leadership must stay connected to a membership, that is quietly saying ‘get us out of this’.
Partner with patient advocacy groups or think tanks to produce reports or proposals that show how better pay and training lead to long-term NHS sustainability.
Prepare for mediation but maintain leverage. If HMG offers mediation, the BMA should accept but demand a binding roadmap.
HMG...
... should publicly acknowledge that early-career doctors have legitimate grievances. Build goodwill by reducing attacks on the BMA, framing demands as greedy.
Validate the idea of pay restoration (at least in part) in the long-term. This will help defuse moral opposition.
Offer a credible, detailed alternative… a multi-year settlement that includes incremental pay restoration tied to system reforms.
Nail in a timetable for non-pay, financial support… loan forgiveness for medical student debt.
Bring in an independent arbiter or mediator (from ACAS or another trusted institution) to broker detailed talks.
Introduce a temporary stability-premium tied to service delivery. Not more basic pay, that’s a red line but a non-consolidated, time-limited recognition payment.
This is ~how the government ended the 2000’s consultants’ dispute and how Agenda for Change deals have been softened.
Emphasise what the Government can and will do, not what it won’t.
Turn a negotiation into a positive narrative about investment in the NHS.
Work together for a Win-Win.
A Joint Task Force… BMA, DHSC, NHSE and external experts to monitor and deliver on commitments. With quarterly public reports.
A Pay and Progression Framework. Tie pay restoration and workforce planning, together.
A Future Doctors' Charter. A publicly communicated document that commits both sides to a long-term settlement… doctors supported, workforce pipeline and career progression.
Agree to commission an independent, expert review of doctor pay, training capacity and retention. Terms of reference that both sides accept… the basis of a legally and politically binding agreement.
If I had to pick one priority for each side?
BMA... secure a binding multi-year roadmap that combines pay restoration with training and career progression. This preserves both leverage and realism.
Government... deliver a detailed, phased offer (pay and non-pay) that is credible to doctors and can be publicly defended.
Reducing the case for further strike action and stabilising the workforce.
Both sides must shift from confrontation to a managed settlement, rooted in realism, mutual recognition and long-term planning.
The alternative is more strikes, bitterness in the workplace, public alienation and long-term damage to NHS morale and capacity...
... in the midst of a chaotic reorganisation, redundancies and a cruel winter.
|