|
Here we go again…
…another review... poking around the undergrowth.
Penny Dash is to lead a review of mental health services... (Who? AKA NHSE Chair)
'... examining productivity, spend and variation...'
Expected to be finished this autumn but may be kept internal... NHSE chair marking NHSE homework is not a good look.
Let’s be clear… this is not a fresh start. The work has been underway for some time. The direction of travel is most likely already set, and…
… for sure, the questions are already known.
Which raises the real issue; is this a review… or a ratification?
That matters.
We don’t lack insight into mental health services. We are drowning in it.
Every report, inquiry and analysis lands in the same place. qwe could write another report right here, now;
-
access is patchy and often too late
- thresholds are inconsistent and sometimes perverse
-
community services are thin and overstretched
-
crisis-care carries too much of the burden
-
the system is fragmented and hard to navigate
-
the service interface with the law and personal freedom, is a Gordian knot
None of that is new. None of it needs rediscovering.
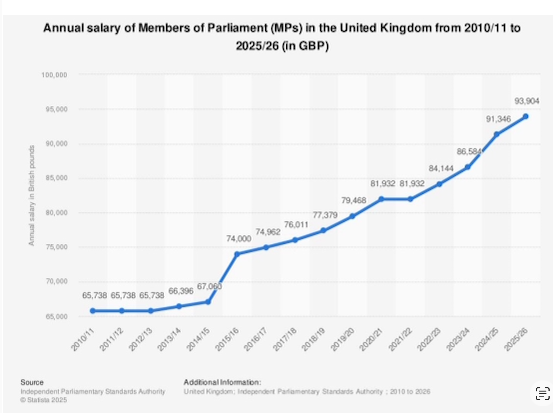
At the same time, a £500m shortfall has opened up as mental health’s share of NHS spending declines.
The past tells us what's what...
... policy says one thing, the pounds in the budgets says another. What will Penny say?
If another review is to be worth the effort, it has to move beyond description and into decisions. That’s where the tension lies.
Dash brings a formidable CV...
... clinical grounding, strategy, regulation, international perspective. She understands variation, waste and system behaviour... seen failure up-close and called it out.
All of that should give us confidence, but…
… her career has also been shaped in the world of analysis, consultancy and system design. A world that is very good at explaining problems, and…
… not always as good at fixing them.
The NHS has a habit of finding work for shelf-makers. Reports neatly racked… gathering dust.
What would make a Dash report any different?
Not another elegant narrative. Not another catalogue of shortcomings. Not another 30 PowerPoint slides.
Instead, just five things.
First, end the threshold lottery.
Patients should not have to deteriorate to qualify for help. A clear, national entitlement… what you get and when.
That would be a start. Without it, the system remains a maze. Particularly for worried families.
Second, shift the centre of gravity.
If community mental health services are the answer, then make them the default.
That means bring money, train the a workforce and land accountability for moving out of hospitals and into neighbourhood teams. Not rhetoric. Redistribution.
Third, integrate for real.
Mental health sits at the intersection of housing, employment, debt and social isolation.
The services with the solutions operate in silos. Is it any wonder it doesn’t work. One plan, one budget, one accountable lead. Otherwise, stop pretending integration is happening.
Fourth, rethink the workforce.
More of the same won’t work. Different skill mixes, new roles, better retention. Burnout and vacancies are not background noise… they’re the main event.
There’s a compelling case for a new kind of practitioner…
…a mental health navigator…
… someone equipped not just with therapeutic skills but with a working knowledge of housing systems, employment support, benefits, debt advice and community resources.
Plus, someone with the skills to introduce the inevitable, AI based support and can give technologies a human interface.
A guide, not a gatekeeper. Someone who can hold the ring, support, stay alongside the patient as they move through a fragmented landscape.
Fifth, measure what matters.
Not just activity and waiting times, but continuity, outcomes and recovery. Otherwise, as ever, we risk hitting targets and missing the point.
Productivity means nothing if people keep coming back.
None of this is revolutionary. That’s the point.
What sits behind much of mental ill-health is not medicine but life;
- work,
- housing,
- debt,
- family strains,
- isolation.
… yet we persist in treating it as if it belongs solely inside clinical services. That’s the risk with ‘just another report’. What’s needed is something sharper.
A willingness to say:
> this is what must change,
> this is where the money goes, and
> this is who is accountable.
Without that, we’re back where we started.
The NHS does not need another review to tell it what it already knows.
It needs the courage to act on what it has known for years.
|