The American Heart Associations Commitment to Research | February is Heart Health Month, a time to highlight the science advancing cardiovascular care. Research funding remains central to the American Heart Association’s lifesaving mission and to the future of heart and stroke medicine. Since 1949, the Association has made sustained investments in research—supporting more than 51,850 projects that have driven breakthroughs in cardiovascular and stroke discovery, translation, and clinical application. To stay informed on the most current findings shaping clinical practice, physicians are encouraged to explore the latest cardiovascular research at the link below. | | |
April 25, 2026
MOA HOUSE OF DELEGATES
MOA Headquarters · Okemos, MI
| |
May 14-17, 2026
MOA SPRING CONFERENCE
Somerset Inn · Troy, MI
| |
June 18-21, 2026
NMOA SUMMER CONFERENCE
Mackinac Island
| |
July 16-19, 2026
AOA HOUSE OF DELEGATES
Chicago, IL
| |
October 23-25, 2026
MOA AUTUMN CONFERENCE
Grand Valley State University - Richard M. DeVos Center
| | ARE YOU INTERESTED IN BECOMING AN OMM MENTOR? | |
The Michigan Osteopathic Association is interested in forming a mentorship program that connects medical students and residents with osteopathic physicians experienced in hands-on training and professional guidance in osteopathic manipulative medicine (OMM).
If you're interested in becoming a mentor, please email Crystal Ash at cash@domoa.org. Thank you for all you DO!
| |
Do you know an outstanding osteopathic resident who deserves recognition?
Consider nominating them for the 2026 MOA Resident of the Year Award.
The MOA seeks to honor a Michigan-based osteopathic resident who exemplifies the highest standards of our profession—someone who goes above and beyond in their work, their service, and their commitment to advancing osteopathic medicine.
Eligible nominees must be in their third year through final year of residency.
One recipient will be announced during the MOA House of Delegates on April 25, 2026. A plaque and a $1,000 award will be presented—or mailed—to the honoree.
NOMINATION DEADLINE: MARCH 3, 2026
| | Live Campus Event Connects Students with MOA Leadership | | |
On Wednesday, February 25, the MOA Student Liaisons will host the annual “Get to Know Your MOA” presentation across all three MSUCOM campuses, offering students a unique opportunity to engage directly with Michigan Osteopathic Association leadership.
This interactive event will feature live speakers on each campus, with a real-time broadcast connecting all locations for a shared panel discussion. Students will be able to interact not only with MOA leaders in person, but also with peers and presenters across campuses during the live discussion.
An MOA leader—including current or past presidents and board members—will be present at each site alongside MOA Student Liaisons. Panelists include MOA President Dr. Adam Hunt, DO, President-Elect Dr. Kevin Beyer, DO, Past President Dr. Andrew Adair, DO, and members of the MOA Board of Trustees, among others.
This annual event is designed to help MSUCOM students better understand the role of the MOA, learn about advocacy and leadership opportunities, and build meaningful connections with the physicians representing them at the state level.
Students are encouraged to attend, ask questions, and take advantage of this opportunity to connect with their MOA.
| | |
| | |
For more than 13 years, the MHA Healthcare Leadership Academy has empowered healthcare professionals to lead with confidence, vision, and impact. This two-part program is designed for healthcare leaders seeking to accelerate their growth and advance their organization’s mission.
| | | | |
In my role as chief medical executive for the State of Michigan, I, Natasha Bagdasarian, MD, MPH, FACP, FIDSA, issue the following standing recommendation under MCL 333.26369:
As of December 18, 2025, health care providers in Michigan should refer to the children’s
vaccine schedules produced by the American Academy of Pediatrics or the American
Academy of Family Physicians, when determining which vaccines their patients should
receive and the timing for their administration.
This recommendation should not supersede clinical judgement in decision making with individual patients.
The Advisory Committee on Immunization Practices (ACIP) was established in 1964 to guide federal vaccine recommendations. While Michigan has previously looked to ACIP’s recommendations, ACIP is an advisory body that Michigan is not bound to follow.
In consultation with the Michigan Department of Health and Human Services Division of Immunizations, I have reviewed current vaccine schedule recommendations produced by the American Academy of Pediatrics (American Academy of Pediatrics 2025 Recommended Child and Adolescent Immunization Schedule for Ages 18 Years or Younger) and the American Academy of Family Physicians (American Academy of Family Physicians, 2025 Birth Through Age 18 Immunization Schedule), and find them to be well-evidenced and based on rigorous review. Employing these schedules will contribute to the advancement of the health of Michigan’s residents and prevent severe, potentially fatal, negative outcomes. I encourage health care providers, health care systems, and health care payers to limit barriers to vaccine access where possible.
| | | | Cost, Community Health Workers, and the Quintuple Aim | |
The Quintuple Aim is a framework developed by the Institute for Healthcare Improvement (IHI, 2025) to understand and improve health system performance. Originally proposed as the Triple Aim in 2012, the framework focused on improving population health, enhancing patient experience, and reducing health care costs. Over time, the model expanded to include other human and equity dimensions of care, resulting in the Quintuple Aim: population health, patient experience, cost, provider well-being, and health equity.
In prior discussions, we explored population health and patient experience, highlighting the essential role Community Health Workers (CHWs) play in delivering high-quality, team-based care. This month, we will discuss cost, which is often considered the most challenging aspect of the Quintuple Aim.
| | What does “cost” mean in the Quintuple Aim? | | |
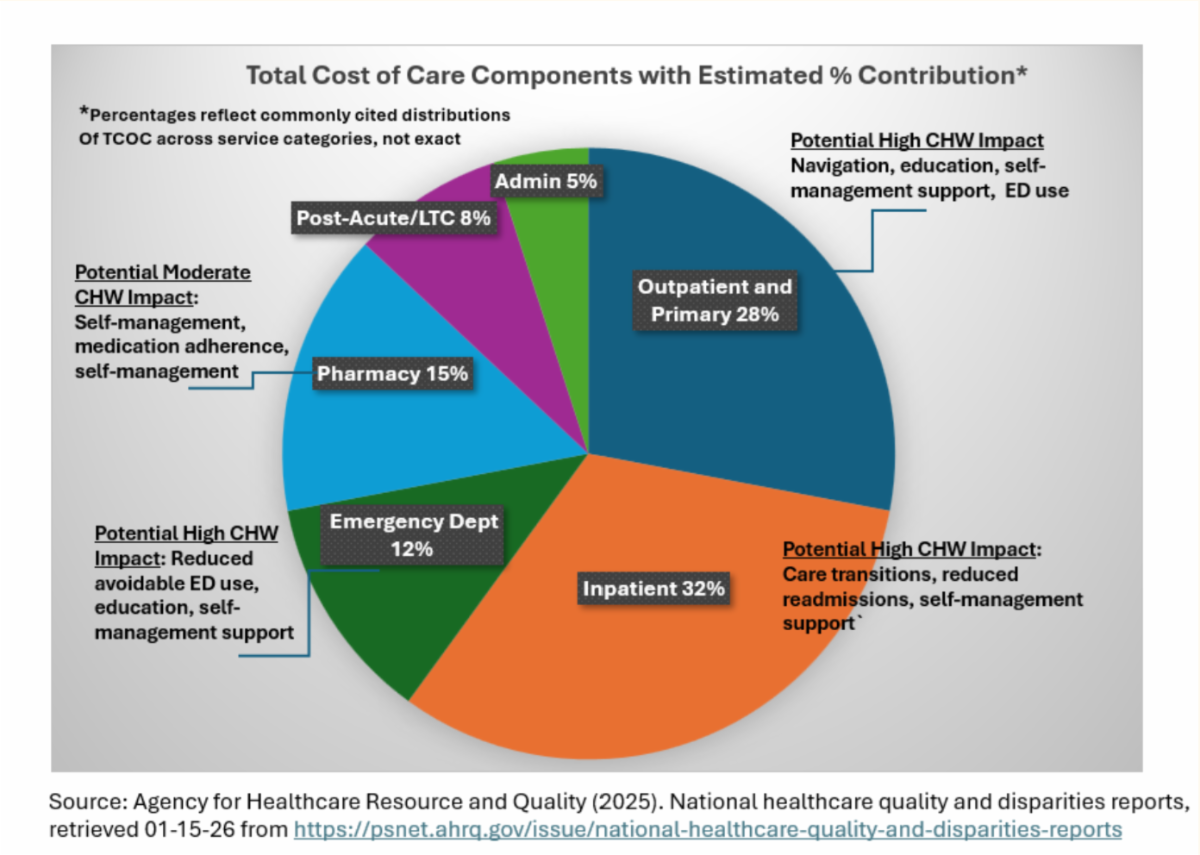
In the context of the Triple Aim, cost refers to the total cost of care for a population. While total cost of care (TCOC) includes the price of services, it is broader and more complex. TCOC includes avoidable emergency department use, inpatient admissions and readmissions, duplication of services (such as tests and medications), inappropriate utilization, and waste caused by inefficiencies.
Increased health care costs place financial strain on patients, families, employers/purchasers, payers, and government programs (e.g., Medicare and Medicaid). The Organisation for Economic Co-operation and Development (OECD) is a group of 37 economically developed member countries that shape policies that foster prosperity, equality, opportunity, and well-being for all (OECD, 2025). The United States has the highest health care cost per capita of all OECD countries. However, this increased spending does not consistently improve outcomes. For example, certain important U.S. health outcomes (life expectancy, maternal mortality, and hospitalizations for heart failure and diabetes) also exceed all OECD countries (Peterson KFF Health Systems Tracker, 2025).
Consistent with the Quintuple Aim and the Chronic Care Model (Wagner, 1998), achieving health care value (decreasing cost while simultaneously improving quality outcomes) will depend on shifting from reactive care to proactive, coordinated, community-based approaches that address utilization drivers.
| Cost ad Social Determinates/drivers of Health (SDOH) | | A significant portion of health care spending is driven by Social Determinants/drivers of Health (SDOH). We often refer to “upstream” and “downstream” care. Downstream care occurs after a problem is identified by treating symptoms and managing associated complications. Upstream care focuses on prevention, root causes, and addressing conditions before illnesses or problems occur. When individuals have unmet SDOH needs (e.g., food insecurity, unstable housing, transportation barriers, lack of access to primary care) they are more likely to delay care and experience worsening chronic conditions. This cycle often results in high-cost services, such as emergency department visits and inpatient admissions where care remains downstream. Moving care upstream will require us to understand how social and environmental factors influence downstream utilization and to invest in strategies to prevent avoidable costs before they occur. | | The role of Community Health Workers (CHWs) in cost reduction | | Community Health Workers (CHWs) play a critical role in advancing the cost dimension of the Quintuple Aim. As we have discussed, CHWs are trusted members of the communities they serve and bridge gaps between clinical care and everyday life. Their lived experience and cultural responsiveness, including using the patient’s primar language, enable CHWs to identify SDOH needs and other barriers to support patients and health teams. The figure below estimates the percentages of TCOC components and potential CHW impact: | | | | |
CHWs help reduce costs by:
- Educating patients on self-management using evidence-base “teach-back,” “show-back,” and motivational interviewing techniques to increase preventive care utilization and reduce inpatient admissions
- Improving follow-up after emergency department visits, redirecting patients to primary care and potentially preventing future inappropriate ED use
- Connecting patients to community-based resources that address SDOH
| | By addressing root causes rather than symptoms alone, CHWs help shift care upstream, improving outcomes while lowering unnecessary utilization and TCOC. | Investing in CHWs as a cost containment strategy | | |
Increasing evidence shows that CHWs are not an added expense but a high-value investment. When integrated effectively into care teams, CHWs contribute to lower utilization, improved quality outcomes, and improved patient and provider experience, advancing multiple dimensions of the Quintuple Aim.
The Practice Transformation Institute (PTI) CHW educational programs are designed to strengthen CHW knowledge, performance, and impact. PTI is an approved provider of Community Health Worker training by the Michigan Department of Health & Human Services (MDHHS), following a rigorous approval process and years of community and health system partnership. PTI is also uniquely distinguished by its IACET accreditation, underscoring its commitment to training excellence.
PTI’s CHW program teaches the nationally recognized C3 Council competencies and equips participants with the skills needed to function effectively across a variety of community and health care settings. This robust training supports CHWs in contributing meaningfully to cost reduction, improved outcomes, and sustainable system transformation.
Investing in prevention, care coordination, and community-based solutions can improve outcomes while managing costs more effectively. CHWs are central to this effort, helping align clinical care with SDOH and other patient eeds to advance the Quintuple Aim in practice.
| |
References
Agency for Healthcare Research and Quality (2025). National healthcare quality and disparities reports. Refer to reference in figure.
Institute for Healthcare Improvement. (2025). The Quintuple Aim.
Organisation for Economic Co-operation and Development (2025). The OECD: Better policies for better lives. Retrieved from https://www.oecd.org/en/about.html
Peterson KFF Health Systems Tracker (2025). How does the quality of the U.S. health system compare to other countries? Retrieved from https://www.healthsystemtracker.org/chart-collection/quality-u-s-healthcare-system-compare-countries/
Wagner, E. H. (1998). Chronic disease management: What will it take to improve care for chronic illness? Effective Clinical Practice, 1, 2–4.
| | |
Clinical Trials Billing Requirements Coming Soon
Effective May 1, we will implement billing guidelines for items and services furnished to members enrolled in approved clinical trials.
Learn More
| |
Medical Record Review Projects
Current and upcoming medical record review projects.
Learn More
| |
The New hap.org is Here – Designed to Support You
Newly redesigned public website is live!
Learn More
| |
HAP Website Launches This Week
Newly redesigned public website going live this week.
Learn More
| |
The Diabetes Care Connection Program - Transforming Diabetes Management for HAP Members
A program designed to support HAP patients at every stage of their diabetes journey.
Learn More
| |
Special Supplemental Benefits for the Chronically Ill Condition Verification
Special Supplemental Benefits for the Chronically Ill (SSBCI) are benefits offered to HAP Medicare Advantage members who have one or more qualifying conditions.
Learn More
| | |
www.cmelearningcenter.com
The Michigan Osteopathic Association (MOA) is committed to the continuum of education and lifelong learning, offering over 150 hours of medical education on-demand. This commitment includes serving as an accredited provider of continuing medical education through the American Osteopathic Association (AOA) to offer AOA Category 1-A Credits. In addition, MOA continues to offer AMA PRA Category 1 Credit(s)TM through a joint providership with the Michigan State University College of Osteopathic Medicine.
| | The Michigan Osteopathic Association partners with several health care organizations to provide resources and job opportunities for physicians at any point in their career. This section offers links to health care organizations and associations who provide information and job postings for DOs. | | | | At McLaren Health Care, our employees help our communities, make life-changing discoveries, and facilitate positive change in health care as a whole. By working for McLaren, you are part of a leading team of talented professionals across many areas of expertise that create a positive difference every day for those we serve. | | | | Mackinac Strait Health System is one of the area’s largest employers, with over 330 team members serving their patients and residents throughout the MSHS organization. Besides offering competitive wages, they also offer an excellent benefits package for full and part time team members, which includes affordable Blue Cross/ Blue Shield Health, Dental and Vision plans, prescription drug plans, generous paid time off, and a defined pension program for your retirement. | | | | At Corewell Health, clinical opportunity intertwines with a commitment to exceptional and personalized care at all levels. Join a clinical team focused on the personalized experience, driving innovation through new technology and achieving national recognition for quality and excellence, all while maintaining the reason you joined this profession—to help people. | | | | Hillsdale Hospital is dedicated to excellence in healthcare community service, continued improvement, and respect for human life. We manage the health needs of our local community through compassionate and highly-skilled care in our clean, safe, healing environment. | | |
Douglas K. Nelson, D.O. | December 31, 2025
Dr. Nelson was a Life Professional who joined the MOA in 1994.
Link to local obituary
Richard Alan Poel, D.O. | December 7, 2025
Dr. Poel was a Life Professional who joined the MOA in 1994.
Link to local obituary
Stuart Willner, D.O. | July 14, 2025
Dr. Willner was a Life Professional who joined the MOA in 1973.
Link to local obituary
Angelo Stoyanovich, D.O. | July 1, 2025
Dr. Stoyanovich joined the MOA in 1981.
Link to local obituary
Lee A. Rea, D.O. | June 21, 2025
Dr. Rea was a Life Professional who joined the MOA in 1971.
Link to local obituary
| | |
Robert Shimmel, D.O. | May 17, 2025
Dr. Shimmel was a Life Professional who joined the MOA in 1957.
Link to local obituary
Roy A. Hills, D.O. | May 5, 2025
Dr. Hills was a Life Professional who joined the MOA in 1954.
Link to local obituary
Kirk Herrick, D.O. | March 2025
Dr. Herrick was an MOA Past President and Life Professional who joined the MOA in 1961.
Gladstone A. Payton, D.O. | Mar 30, 2025
Dr. Payton was a Life Professional who joined the MOA in 1969.
Link to local obituary
| | | | |